Take the April 2025 Warning Letter to Cosco International, for example. One might quickly react with, “Holy cow! No process validation or cleaning validation—how is this even possible?” This could spark an exhaustive discussion about why these regulations have been in place for 30 years and the urgent need for companies to comply. But frankly, nothing really valuable to a company that already realizes they need to do process validation.
Yet this Warning Letter highlights a fundamental misunderstanding among companies regarding the difference between a cosmetic and a drug. As someone who reads Warning Letters, this seems to be a fairly common problem.
Key Regulatory Distinctions
Cosmetics: Products intended solely for cleansing, beautifying, or altering the appearance without affecting bodily functions are regulated as cosmetics under the FDA. These are not required to undergo premarket approval, except for color additives.
Drugs: Products intended to diagnose, cure, mitigate, treat, or prevent disease or that affect the structure or function of the body (such as blocking sweat glands) are regulated as drugs. This includes antiperspirants, regardless of their application site.
So not really all that interesting from a biotech perspective, but a fascinating insight to some bad trends if I was on the consumer goods side of the profession.
But, as I discussed, there is value from reading these holistically, for what they tell us regulators are thinking. In this case, there is a nice little set of bullet points on what is bare minimum in cleaning validation.
The FDA’s April 30, 2025 warning letter to Rechon Life Science AB serves as a great learning opportunity about the importance robust investigation systems to contamination control to drive meaningful improvements. This Swedish contract manufacturer’s experience offers profound lessons for quality professionals navigating the intersection of EU Annex 1‘s contamination control strategy requirements and increasingly regulatory expectations. It is a mistake to think that just because the FDA doesn’t embrace the prescriptive nature of Annex 1 the agency is not fully aligned with the intent.
This Warning Letter resonates with similar systemic failures at companies like LeMaitre Vascular, Sanofi and others. The Rechon warning letter demonstrates a troubling but instructive pattern: organizations that fail to conduct meaningful contamination investigations inevitably find themselves facing regulatory action that could have been prevented through better investigation practices and systematic contamination control approaches.
The Cascade of Investigation Failures: Rechon’s Contamination Control Breakdown
Aseptic Process Failures and the Investigation Gap
Rechon’s primary violation centered on a fundamental breakdown in aseptic processing—operators were routinely touching critical product contact surfaces with gloved hands, a practice that was not only observed but explicitly permitted in their standard operating procedures. This represents more than poor technique; it reveals an organization that had normalized contamination risks through inadequate investigation and assessment processes.
The FDA’s citation noted that Rechon failed to provide environmental monitoring trend data for surface swab samples, representing exactly the kind of “aspirational data” problem. When investigation systems don’t capture representative information about actual manufacturing conditions, organizations operate in a state of regulatory blindness, making decisions based on incomplete or misleading data.
This pattern reflects a broader failure in contamination investigation methodology: environmental monitoring excursions require systematic evaluation that includes all environmental data (i.e. viable and non-viable tests) and must include areas that are physically adjacent or where related activities are performed. Rechon’s investigation gaps suggest they lacked these fundamental systematic approaches.
Environmental Monitoring Investigations: When Trend Analysis Fails
Perhaps more concerning was Rechon’s approach to persistent contamination with objectionable microorganisms—gram-negative organisms and spore formers—in ISO 5 and 7 areas since 2022. Their investigation into eight occurrences of gram-negative organisms concluded that the root cause was “operators talking in ISO 7 areas and an increase of staff illness,” a conclusion that demonstrates fundamental misunderstanding of contamination investigation principles.
As an aside, ISO7/Grade C is not normally an area we see face masks.
Effective investigations must provide comprehensive evaluation including:
Background and chronology of events with detailed timeline analysis
Investigation and data gathering activities including interviews and training record reviews
SME assessments from qualified microbiology and manufacturing science experts
Historical data review and trend analysis encompassing the full investigation zone
Manufacturing process assessment to determine potential contributing factors
Environmental conditions evaluation including HVAC, maintenance, and cleaning activities
Rechon’s investigation lacked virtually all of these elements, focusing instead on convenient behavioral explanations that avoided addressing systematic contamination sources. The persistence of gram-negative organisms and spore formers over a three-year period represented a clear adverse trend requiring a comprehensive investigation approach.
The Annex 1 Contamination Control Strategy Imperative: Beyond Compliance to Integration
The Paradigm Shift in Contamination Control
The revised EU Annex 1, effective since August 2023 demonstrates the current status of regulatory expectations around contamination control, moving from isolated compliance activities toward integrated risk management systems. The mandatory Contamination Control Strategy (CCS) requires manufacturers to develop comprehensive, living documents that integrate all aspects of contamination risk identification, mitigation, and monitoring.
Industry implementation experience since 2023 has revealed that many organizations are faiing to make meaningful connections between existing quality systems and the Annex 1 CCS requirements. Organizations struggle with the time and resource requirements needed to map existing contamination controls into coherent strategies, which often leads to discovering significant gaps in their understanding of their own processes.
Representative Environmental Monitoring Under Annex 1
The updated guidelines place emphasis on continuous monitoring and representative sampling that reflects actual production conditions rather than idealized scenarios. Rechon’s failure to provide comprehensive trend data demonstrates exactly the kind of gap that Annex 1 was designed to address.
Environmental monitoring must function as part of an integrated knowledge system that combines explicit knowledge (documented monitoring data, facility design specifications, cleaning validation reports) with tacit knowledge about facility-specific contamination risks and operational nuances. This integration demands investigation systems capable of revealing actual contamination patterns rather than providing comfortable explanations for uncomfortable realities.
The Design-First Philosophy
One of Annex 1’s most significant philosophical shifts is the emphasis on design-based contamination control rather than monitoring-based approaches. As we see from Warning Letters, and other regulatory intelligence, design gaps are frequently being cited as primary compliance failures, reinforcing the principle that organizations cannot monitor or control their way out of poor design.
This design-first philosophy fundamentally changes how contamination investigations must be conducted. Instead of simply investigating excursions after they occur, robust investigation systems must evaluate whether facility and process designs create inherent contamination risks that make excursions inevitable. Rechon’s persistent contamination issues suggest their investigation systems never addressed these fundamental design questions.
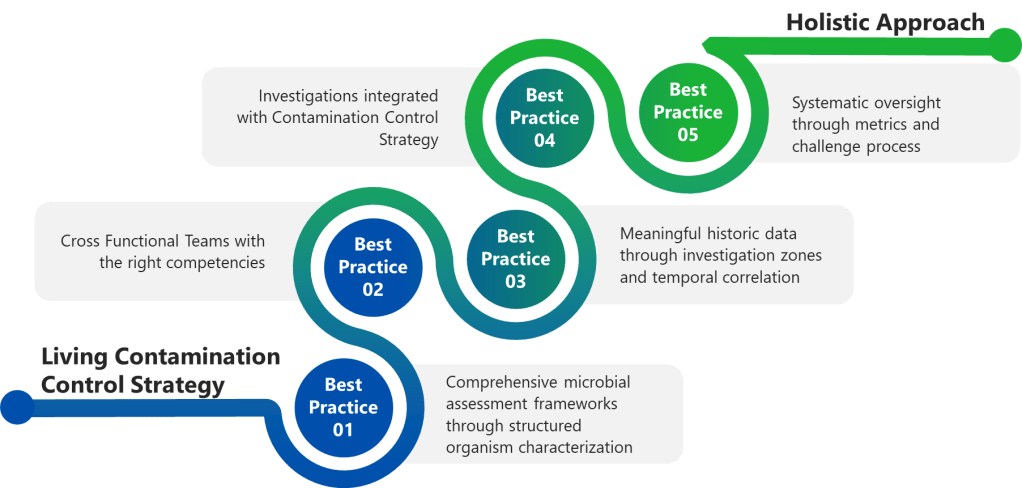
Best Practice 1: Implement Comprehensive Microbial Assessment Frameworks
Structured Organism Characterization
Effective contamination investigations begin with proper microbial assessments that characterize organisms based on actual risk profiles rather than convenient categorizations.
Complete microorganism documentation encompassing organism type, Gram stain characteristics, potential sources, spore-forming capability, and objectionable organism status. The structured approach outlined in formal assessment templates ensures consistent evaluation across different sample types (in-process, environmental monitoring, water and critical utilities).
Quantitative occurrence assessment using standardized vulnerability scoring systems that combine occurrence levels (Low, Medium, High) with nature and history evaluations. This matrix approach prevents investigators from minimizing serious contamination events through subjective assessments.
Severity evaluation based on actual manufacturing impact rather than theoretical scenarios. For environmental monitoring excursions, severity assessments must consider whether microorganisms were detected in controlled environments during actual production activities, the potential for product contamination, and the effectiveness of downstream processing steps.
Risk determination through systematic integration of vulnerability scores and severity ratings, providing objective classification of contamination risks that drives appropriate corrective action responses.
Rechon’s superficial investigation approach suggests they lacked these systematic assessment frameworks, focusing instead on behavioral explanations that avoided comprehensive organism characterization and risk assessment.
Best Practice 2: Establish Cross-Functional Investigation Teams with Defined Competencies
Investigation Team Composition and Qualifications
Major contamination investigations require dedicated cross-functional teams with clearly defined responsibilities and demonstrated competencies. The investigation lead must possess not only appropriate training and experience but also technical knowledge of the process and cGMP/quality system requirements, and ability to apply problem-solving tools.
Minimum team composition requirements for major investigations must include:
Impacted Department representatives (Manufacturing, Facilities) with direct operational knowledge
Subject Matter Experts (Manufacturing Sciences and Technology, QC Microbiology) with specialized technical expertise
Contamination Control specialists serving as Quality Assurance approvers with regulatory and risk assessment expertise
Investigation scope requirements must encompass systematic evaluation including background/chronology documentation, comprehensive data gathering activities (interviews, training record reviews), SME assessments, impact statement development, historical data review and trend analysis, and laboratory investigation summaries.
Training and Competency Management
Investigation team effectiveness depends on systematic competency development and maintenance. Teams must demonstrate proficiency in:
Root cause analysis methodologies including fishbone analysis, why-why questioning, fault tree analysis, and failure mode and effects analysis approaches suited to contamination investigation contexts.
Contamination microbiology principles including organism identification, source determination, growth condition assessment, and disinfectant efficacy evaluation specific to pharmaceutical manufacturing environments.
Risk assessment and impact evaluation capabilities that can translate investigation findings into meaningful product, process, and equipment risk determinations.
Regulatory requirement understanding encompassing both domestic and international contamination control expectations, investigation documentation standards, and CAPA development requirements.
The superficial nature of Rechon’s gram-negative organism investigation suggests their teams lacked these fundamental competencies, resulting in conclusions that satisfied neither regulatory expectations nor contamination control best practices.
Best Practice 3: Conduct Meaningful Historical Data Review and Comprehensive Trend Analysis
Investigation Zone Definition and Data Integration
Effective contamination investigations require comprehensive trend analysis that extends beyond simple excursion counting to encompass systematic pattern identification across related operational areas. As established in detailed investigation procedures, historical data review must include:
Physically adjacent areas and related activities recognition that contamination events rarely occur in isolation. Processing activities spanning multiple rooms, secondary gowning areas leading to processing zones, material transfer airlocks, and all critical utility distribution points must be included in investigation zones.
Comprehensive environmental data analysis encompassing all environmental data (i.e. viable and non-viable tests) to identify potential correlations between different contamination indicators that might not be apparent when examining single test types in isolation.
Extended historical review capabilities for situations where limited or no routine monitoring was performed during the questioned time frame, requiring investigation teams to expand their analytical scope to capture relevant contamination patterns.
Microorganism identification pattern assessment to determine shifts in routine microflora or atypical or objectionable organisms, enabling detection of contamination source changes that might indicate facility or process deterioration.
Temporal Correlation Analysis
Sophisticated trend analysis must correlate contamination events with operational activities, environmental conditions, and facility modifications that might contribute to adverse trends:
Manufacturing activity correlation examining whether contamination patterns correlate with specific production campaigns, personnel schedules, cleaning activities, or maintenance operations that might introduce contamination sources.
Environmental condition assessment including HVAC system performance, pressure differential maintenance, temperature and humidity control, and compressed air quality that could influence contamination recovery patterns.
Facility modification impact evaluation determining whether physical environment changes, equipment installations, utility upgrades, or process modifications correlate with contamination trend emergence or intensification.
Rechon’s three-year history of gram-negative and spore-former recovery represented exactly the kind of adverse trend requiring this comprehensive analytical approach. Their failure to conduct meaningful trend analysis prevented identification of systematic contamination sources that behavioral explanations could never address.
Best Practice 4: Integrate Investigation Findings with Dynamic Contamination Control Strategy
Knowledge Management and CCS Integration
Under Annex 1 requirements, investigation findings must feed directly into the overall Contamination Control Strategy, creating continuous improvement cycles that enhance contamination risk understanding and control effectiveness. This integration requires sophisticated knowledge management systems that capture both explicit investigation data and tacit operational insights.
Explicit knowledge integration encompasses formal investigation reports, corrective action documentation, trending analysis results, and regulatory correspondence that must be systematically incorporated into CCS risk assessments and control measure evaluations.
Tacit knowledge capture including personnel experiences with contamination events, operational observations about facility or process vulnerabilities, and institutional understanding about contamination source patterns that may not be fully documented but represent critical CCS inputs.
Risk Assessment Dynamic Updates
CCS implementation demands that investigation findings trigger systematic risk assessment updates that reflect enhanced understanding of contamination vulnerabilities:
Contamination source identification updates based on investigation findings that reveal previously unrecognized or underestimated contamination pathways requiring additional control measures or monitoring enhancements.
Control measure effectiveness verification through post-investigation monitoring that demonstrates whether implemented corrective actions actually reduce contamination risks or require further enhancement.
Monitoring program optimization based on investigation insights about contamination patterns that may indicate needs for additional sampling locations, modified sampling frequencies, or enhanced analytical methods.
Continuous Improvement Integration
The CCS must function as a living document that evolves based on investigation findings rather than remaining static until the next formal review cycle:
Investigation-driven CCS updates that incorporate new contamination risk understanding into facility design assessments, process control evaluations, and personnel training requirements.
Performance metrics integration that tracks investigation quality indicators alongside traditional contamination control metrics to ensure investigation systems themselves contribute to contamination risk reduction.
Cross-site knowledge sharing mechanisms that enable investigation insights from one facility to enhance contamination control strategies at related manufacturing sites.
Best Practice 5: Establish Investigation Quality Metrics and Systematic Oversight
Investigation Completeness and Quality Assessment
Organizations must implement systematic approaches to ensure investigation quality and prevent the superficial analysis demonstrated by Rechon. This requires comprehensive quality metrics that evaluate both investigation process compliance and outcome effectiveness:
Investigation completeness verification using a rubric or other standardized checklists that ensure all required investigation elements have been addressed before investigation closure. These must verify background documentation adequacy, data gathering comprehensiveness, SME assessment completion, impact evaluation thoroughness, and corrective action appropriateness.
Root cause determination quality assessment evaluating whether investigation conclusions demonstrate scientific rigor and logical connection between identified causes and observed contamination events. This includes verification that root cause analysis employed appropriate methodologies and that conclusions can withstand independent technical review.
Corrective action effectiveness verification through systematic post-implementation monitoring that demonstrates whether corrective actions achieved their intended contamination risk reduction objectives.
Management Review and Challenge Processes
Effective investigation oversight requires management systems that actively challenge investigation conclusions and ensure scientific rationale supports all determinations:
Technical review panels comprising independent SMEs who evaluate investigation methodology, data interpretation, and conclusion validity before investigation closure approval for major and critical deviations. I strongly recommend this as part of qualification and re-qualification activities.
Regulatory perspective integration ensuring investigation approaches and conclusions align with current regulatory expectations and enforcement trends rather than relying on outdated compliance interpretations.
Cross-functional impact assessment verifying that investigation findings and corrective actions consider all affected operational areas and don’t create unintended contamination risks in other facility areas.
CAPA System Integration and Effectiveness Tracking
Investigation findings must integrate with robust CAPA systems that ensure systematic improvements rather than isolated fixes:
Systematic improvement identification that links investigation findings to broader facility or process enhancement opportunities rather than limiting corrective actions to immediate excursion sources.
CAPA implementation quality management including resource allocation verification, timeline adherence monitoring, and effectiveness verification protocols that ensure corrective actions achieve intended risk reduction.
Knowledge management integration that captures investigation insights for application to similar contamination risks across the organization and incorporates lessons learned into training programs and preventive maintenance activities.
Rechon’s continued contamination issues despite previous investigations suggest their CAPA processes lacked this systematic improvement approach, treating each contamination event as isolated rather than symptoms of broader contamination control weaknesses.
The Investigation-Annex 1 Integration Challenge: Building Investigation Resilience
Holistic Contamination Risk Assessment
Contamination control requires investigation systems that function as integral components of comprehensive strategies rather than reactive compliance activities.
Design-Investigation Integration demands that investigation findings inform facility design assessments and process modification evaluations. When investigations reveal design-related contamination sources, CCS updates must address whether facility modifications or process changes can eliminate contamination risks at their source rather than relying on monitoring and control measures.
Process Knowledge Enhancement through investigation activities that systematically build organizational understanding of contamination vulnerabilities, control measure effectiveness, and operational factors that influence contamination risk profiles.
Personnel Competency Development that leverages investigation findings to identify training needs, competency gaps, and behavioral factors that contribute to contamination risks requiring systematic rather than individual corrective approaches.
Technology Integration and Future Investigation Capabilities
Advanced Monitoring and Investigation Support Systems
The increasing sophistication of regulatory expectations necessitates corresponding advances in investigation support technologies that enable more comprehensive and efficient contamination risk assessment:
Real-time monitoring integration that provides investigation teams with comprehensive environmental data streams enabling correlation analysis between contamination events and operational variables that might not be captured through traditional discrete sampling approaches.
Automated trend analysis capabilities that identify contamination patterns and correlations across multiple data sources, facility areas, and time periods that might not be apparent through manual analysis methods.
Integrated knowledge management platforms that capture investigation insights, corrective action outcomes, and operational observations in formats that enable systematic application to future contamination risk assessments and control strategy optimization.
Investigation Standardization and Quality Enhancement
Technology solutions must also address investigation process standardization and quality improvement:
Investigation workflow management systems that ensure consistent application of investigation methodologies, prevent shortcuts that compromise investigation quality, and provide audit trails demonstrating compliance with regulatory expectations.
Cross-site investigation coordination capabilities that enable investigation insights from one facility to inform contamination risk assessments and investigation approaches at related manufacturing sites.
Building Organizational Investigation Excellence
Cultural Transformation Requirements
The evolution from compliance-focused contamination investigations toward risk-based contamination control strategies requires fundamental cultural changes that extend beyond procedural updates:
Leadership commitment demonstration through resource allocation for investigation system enhancement, personnel competency development, and technology infrastructure investment that enables comprehensive contamination risk assessment rather than minimal compliance achievement.
Cross-functional collaboration enhancement that breaks down organizational silos preventing comprehensive investigation approaches and ensures investigation teams have access to all relevant operational expertise and information sources.
Continuous improvement mindset development that views contamination investigations as opportunities for systematic facility and process enhancement rather than unfortunate compliance burdens to be minimized.
Investigation as Strategic Asset
Organizations that excel in contamination investigation develop capabilities that provide competitive advantages beyond regulatory compliance:
Process optimization opportunities identification through investigation activities that reveal operational inefficiencies, equipment performance issues, and facility design limitations that, when addressed, improve both contamination control and operational effectiveness.
Risk management capability enhancement that enables proactive identification and mitigation of contamination risks before they result in regulatory scrutiny or product quality issues requiring costly remediation.
Regulatory relationship management through demonstration of investigation competence and commitment to continuous improvement that can influence regulatory inspection frequency and focus areas.
The Cost of Investigation Mediocrity: Lessons from Enforcement
Regulatory Consequences and Business Impact
Rechon’s experience demonstrates the ultimate cost of inadequate contamination investigations: comprehensive regulatory action that threatens market access and operational continuity. The FDA’s requirements for extensive remediation—including independent assessment of investigation systems, comprehensive personnel and environmental monitoring program reviews, and retrospective out-of-specification result analysis—represent exactly the kind of work that should be conducted proactively rather than reactively.
Resource Allocation and Opportunity Cost
The remediation requirements imposed on companies receiving warning letters far exceed the resource investment required for proactive investigation system development:
Independent consultant engagement costs for comprehensive facility and system assessment that could be avoided through internal investigation capability development and systematic contamination control strategy implementation.
Production disruption resulting from regulatory holds, additional sampling requirements, and corrective action implementation that interrupts normal manufacturing operations and delays product release.
Market access limitations including potential product recalls, import restrictions, and regulatory approval delays that affect revenue streams and competitive positioning.
Reputation and Trust Impact
Beyond immediate regulatory and financial consequences, investigation failures create lasting reputation damage that affects customer relationships, regulatory standing, and business development opportunities:
Customer confidence erosion when investigation failures become public through warning letters, regulatory databases, and industry communications that affect long-term business relationships.
Regulatory relationship deterioration that can influence future inspection focus areas, approval timelines, and enforcement approaches that extend far beyond the original contamination control issues.
Industry standing impact that affects ability to attract quality personnel, develop partnerships, and maintain competitive positioning in increasingly regulated markets.
Gap Assessment Framework: Organizational Investigation Readiness
Investigation System Evaluation Criteria
Organizations should systematically assess their investigation capabilities against current regulatory expectations and best practice standards. This assessment encompasses multiple evaluation dimensions:
Technical Competency Assessment
Do investigation teams possess demonstrated expertise in contamination microbiology, facility design, process engineering, and regulatory requirements?
Are investigation methodologies standardized, documented, and consistently applied across different contamination scenarios?
Does investigation scope routinely include comprehensive trend analysis, adjacent area assessment, and environmental correlation analysis?
Are investigation conclusions supported by scientific rationale and independent technical review?
Resource Adequacy Evaluation
Are sufficient personnel resources allocated to enable comprehensive investigation completion within reasonable timeframes?
Do investigation teams have access to necessary analytical capabilities, reference materials, and technical support resources?
Are investigation budgets adequate to support comprehensive data gathering, expert consultation, and corrective action implementation?
Does management demonstrate commitment through resource allocation and investigation priority establishment?
Integration and Effectiveness Assessment
Are investigation findings systematically integrated into contamination control strategy updates and facility risk assessments?
Do CAPA systems ensure investigation insights drive systematic improvements rather than isolated fixes?
Are investigation outcomes tracked and verified to confirm contamination risk reduction achievement?
Do knowledge management systems capture and apply investigation insights across the organization?
From Investigation Adequacy to Investigation Excellence
Rechon Life Science’s experience serves as a cautionary tale about the consequences of investigation mediocrity, but it also illustrates the transformation potential inherent in comprehensive contamination control strategy implementation. When organizations invest in systematic investigation capabilities—encompassing proper team composition, comprehensive analytical approaches, effective knowledge management, and continuous improvement integration—they build competitive advantages that extend far beyond regulatory compliance.
The key insight emerging from regulatory enforcement patterns is that contamination control has evolved from a specialized technical discipline into a comprehensive business capability that affects every aspect of pharmaceutical manufacturing. The quality of an organization’s contamination investigations often determines whether contamination events become learning opportunities that strengthen operations or regulatory nightmares that threaten business continuity.
For quality professionals responsible for contamination control, the message is unambiguous: investigation excellence is not an optional enhancement to existing compliance programs—it’s a fundamental requirement for sustainable pharmaceutical manufacturing in the modern regulatory environment. The organizations that recognize this reality and invest accordingly will find themselves well-positioned not only for regulatory success but for operational excellence that drives competitive advantage in increasingly complex global markets.
The regulatory landscape has fundamentally changed, and traditional approaches to contamination investigation are no longer sufficient. Organizations must decide whether to embrace the investigation excellence imperative or face the consequences of continuing with approaches that regulatory agencies have clearly indicated are inadequate. The choice is clear, but the window for proactive transformation is narrowing as regulatory expectations continue to evolve and enforcement intensifies.
The question facing every pharmaceutical manufacturer is not whether contamination control investigations will face increased scrutiny—it’s whether their investigation systems will demonstrate the excellence necessary to transform regulatory challenges into competitive advantages. Those that choose investigation excellence will thrive; those that don’t will join Rechon Life Science and others in explaining their investigation failures to regulatory agencies rather than celebrating their contamination control successes in the marketplace.
The FDA’s August 11, 2025 warning letter to LeMaitre Vascular reads like a masterclass in how fundamental water system deficiencies can cascade into comprehensive quality system failures. This warning letter offers lessons about the interconnected nature of pharmaceutical water systems and the regulatory expectations that surround them.
The Foundation Cracks
What makes this warning letter particularly instructive is how it demonstrates that water systems aren’t just utilities—they’re critical manufacturing infrastructure whose failures ripple through every aspect of product quality. LeMaitre’s North Brunswick facility, which manufactures Artegraft Collagen Vascular Grafts, found itself facing six major violations, with water system inadequacies serving as the primary catalyst.
The Artegraft device itself—a bovine carotid artery graft processed through enzymatic digestion and preserved in USP purified water and ethyl alcohol—places unique demands on water system reliability. When that foundation fails, everything built upon it becomes suspect.
Water Sampling: The Devil in the Details
The first violation strikes at something discussed extensively in previous posts: representative sampling. LeMaitre’s USP water sampling procedures contained what the FDA termed “inconsistent and conflicting requirements” that fundamentally compromised the representativeness of their sampling.
Consider the regulatory expectation here. As outlined in ISPE guideline, “sampling a POU must include any pathway that the water travels to reach the process”. Yet LeMaitre was taking samples through methods that included purging, flushing, and disinfection steps that bore no resemblance to actual production use. This isn’t just a procedural misstep—it’s a fundamental misunderstanding of what water sampling is meant to accomplish.
The FDA’s criticism centers on three critical sampling failures:
Sampling Location Discrepancies: Taking samples through different pathways than production water actually follows. This violates the basic principle that quality control sampling should “mimic the way the water is used for manufacturing”.
Pre-Sampling Conditioning: The procedures required extensive purging and cleaning before sampling—activities that would never occur during normal production use. This creates “aspirational data”—results that reflect what we wish our system looked like rather than how it actually performs.
Inconsistent Documentation: Failure to document required replacement activities during sampling, creating gaps in the very records meant to demonstrate control.
The Sterilant Switcheroo
Perhaps more concerning was LeMaitre’s unauthorized change of sterilant solutions for their USP water system sanitization. The company switched sterilants sometime in 2024 without documenting the change control, assessing biocompatibility impacts, or evaluating potential contaminant differences.
This represents a fundamental failure in change control—one of the most basic requirements in pharmaceutical manufacturing. Every change to a validated system requires formal assessment, particularly when that change could affect product safety. The fact that LeMaitre couldn’t provide documentation allowing for this change during inspection suggests a broader systemic issue with their change control processes.
Environmental Monitoring: Missing the Forest for the Trees
The second major violation addressed LeMaitre’s environmental monitoring program—specifically, their practice of cleaning surfaces before sampling. This mirrors issues we see repeatedly in pharmaceutical manufacturing, where the desire for “good” data overrides the need for representative data.
Environmental monitoring serves a specific purpose: to detect contamination that could reasonably be expected to occur during normal operations. When you clean surfaces before sampling, you’re essentially asking, “How clean can we make things when we try really hard?” rather than “How clean are things under normal operating conditions?”
The regulatory expectation is clear: environmental monitoring should reflect actual production conditions, including normal personnel traffic and operational activities. LeMaitre’s procedures required cleaning surfaces and minimizing personnel traffic around air samplers—creating an artificial environment that bore little resemblance to actual production conditions.
Sterilization Validation: Building on Shaky Ground
The third violation highlighted inadequate sterilization process validation for the Artegraft products. LeMaitre failed to consider bioburden of raw materials, their storage conditions, and environmental controls during manufacturing—all fundamental requirements for sterilization validation.
This connects directly back to the water system failures. When your water system monitoring doesn’t provide representative data, and your environmental monitoring doesn’t reflect actual conditions, how can you adequately assess the bioburden challenges your sterilization process must overcome?
The FDA noted that LeMaitre had six out-of-specification bioburden results between September 2024 and March 2025, yet took no action to evaluate whether testing frequency should be increased. This represents a fundamental misunderstanding of how bioburden data should inform sterilization validation and ongoing process control.
CAPA: When Process Discipline Breaks Down
The final violations addressed LeMaitre’s Corrective and Preventive Action (CAPA) system, where multiple CAPAs exceeded their own established timeframes by significant margins. A high-risk CAPA took 81 days instead of the required timeframe, while medium and low-risk CAPAs exceeded deadlines by 120-216 days.
This isn’t just about missing deadlines—it’s about the erosion of process discipline. When CAPA systems lose their urgency and rigor, it signals a broader cultural issue where quality requirements become suggestions rather than requirements.
The Recall That Wasn’t
Perhaps most concerning was LeMaitre’s failure to report a device recall to the FDA. The company distributed grafts manufactured using raw material from a non-approved supplier, with one graft implanted in a patient before the recall was initiated. This constituted a reportable removal under 21 CFR Part 806, yet LeMaitre failed to notify the FDA as required.
This represents the ultimate failure: when quality system breakdowns reach patients. The cascade from water system failures to inadequate environmental monitoring to poor change control ultimately resulted in a product safety issue that required patient intervention.
Gap Assessment Questions
For organizations conducting their own gap assessments based on this warning letter, consider these critical questions:
Water System Controls
Are your water sampling procedures representative of actual production use conditions?
Do you have documented change control for any modifications to water system sterilants or sanitization procedures?
Are all water system sampling activities properly documented, including any maintenance or replacement activities?
Have you assessed the impact of any sterilant changes on product biocompatibility?
Environmental Monitoring
Do your environmental monitoring procedures reflect normal production conditions?
Are surfaces cleaned before environmental sampling, and if so, is this representative of normal operations?
Does your environmental monitoring capture the impact of actual personnel traffic and operational activities?
Are your sampling frequencies and locations justified by risk assessment?
Sterilization and Bioburden Control
Does your sterilization validation consider bioburden from all raw materials and components?
Have you established appropriate bioburden testing frequencies based on historical data and risk assessment?
Do you have procedures for evaluating when bioburden testing frequency should be increased based on out-of-specification results?
Are bioburden results from raw materials and packaging components included in your sterilization validation?
CAPA System Integrity
Are CAPA timelines consistently met according to your established procedures?
Do you have documented rationales for any CAPA deadline extensions?
Is CAPA effectiveness verification consistently performed and documented?
Are supplier corrective actions properly tracked and their effectiveness verified?
Change Control and Documentation
Are all changes to validated systems properly documented and assessed?
Do you have procedures for notifying relevant departments when suppliers change materials or processes?
Are the impacts of changes on product quality and safety systematically evaluated?
Is there a formal process for assessing when changes require revalidation?
Regulatory Compliance
Are all required reports (corrections, removals, MDRs) submitted within regulatory timeframes?
Do you have systems in place to identify when product removals constitute reportable events?
Are all regulatory communications properly documented and tracked?
Learning from LeMaitre’s Missteps
This warning letter serves as a reminder that pharmaceutical manufacturing is a system of interconnected controls, where failures in fundamental areas like water systems can cascade through every aspect of operations. The path from water sampling deficiencies to patient safety issues is shorter than many organizations realize.
The most sobering aspect of this warning letter is how preventable these violations were. Representative sampling, proper change control, and timely CAPA completion aren’t cutting-edge regulatory science—they’re fundamental GMP requirements that have been established for decades.
For quality professionals, this warning letter reinforces the importance of treating utility systems with the same rigor we apply to manufacturing processes. Water isn’t just a raw material—it’s a critical quality attribute that deserves the same level of control, monitoring, and validation as any other aspect of your manufacturing process.
The question isn’t whether your water system works when everything goes perfectly. The question is whether your monitoring and control systems will detect problems before they become patient safety issues. Based on LeMaitre’s experience, that’s a question worth asking—and answering—before the FDA does it for you.
The recently released draft of ICH Q3E addresses a critical gap that has persisted in pharmaceutical regulation for over two decades. Since the FDA’s 1999 Container Closure Systems guidance and the EMA’s 2005 Plastic Immediate Packaging Materials guideline, the regulatory landscape for extractables and leachables has remained fragmented across regions and dosage forms. This fragmentation has created significant challenges for global pharmaceutical companies, leading to inconsistent approaches, variable interpretation of requirements, and substantial regulatory uncertainty that ultimately impacts patient access to medicines.
The ICH Q3E guideline emerges from recognition that modern pharmaceutical development increasingly relies on complex drug-device combinations, novel delivery systems, and sophisticated manufacturing technologies that transcend traditional regulatory boundaries. Biologics, cell and gene therapies, combination products, and single-use manufacturing systems have created E&L challenges that existing guidance documents were never designed to address. The guideline’s comprehensive scope encompasses chemical entities, biologics, biotechnological products, and drug-device combinations across all dosage forms, establishing a unified framework that reflects the reality of contemporary pharmaceutical manufacturing.
The harmonization achieved through ICH Q3E extends beyond mere procedural alignment to establish fundamental scientific principles that can be applied consistently regardless of geographical location or specific regulatory jurisdiction. This represents a significant evolution from the current patchwork of guidance documents, each with distinct requirements and safety thresholds that often conflict or create unnecessary redundancy in global development programs.
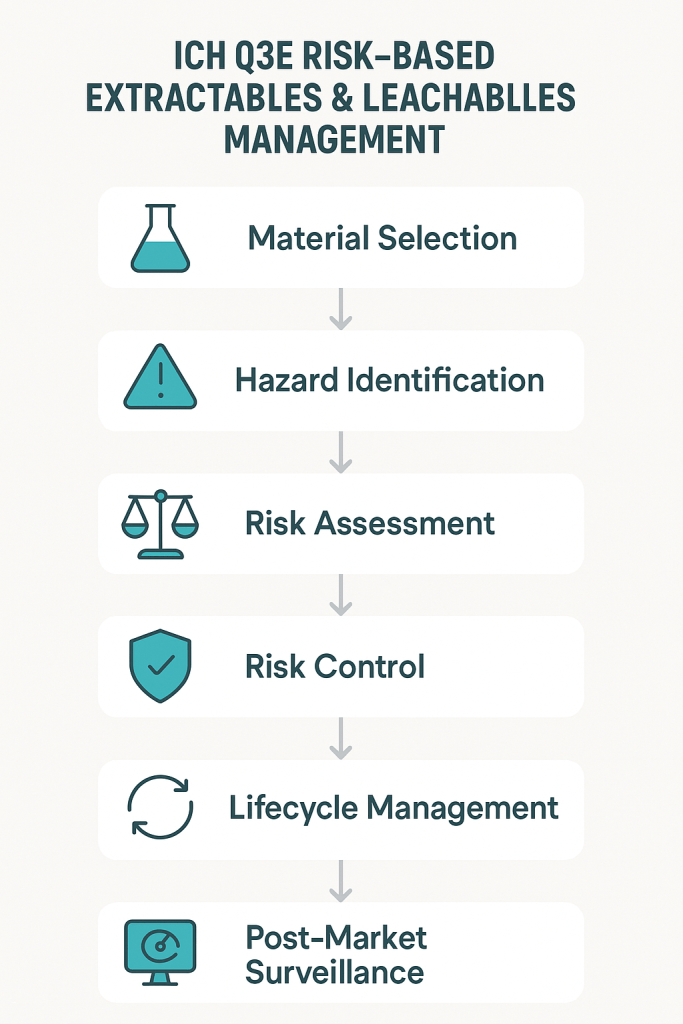
The most transformative aspect of ICH Q3E lies in its integration of comprehensive risk management principles derived from ICH Q9 throughout the entire E&L assessment process. This represents a fundamental departure from the prescriptive, one-size-fits-all approaches that have characterized previous guidance documents. The risk management framework encompasses four critical stages: hazard identification, risk assessment, risk control, and lifecycle management.
The hazard identification phase requires systematic evaluation of all materials of construction, manufacturing processes, and storage conditions that could contribute to extractables formation or leachables migration. This includes not only primary packaging components but also manufacturing equipment, single-use systems, filters, tubing, and any other materials that contact the drug substance or drug product during production, storage, or administration. The guideline recognizes that modern pharmaceutical manufacturing involves complex material interactions that require comprehensive evaluation beyond traditional container-closure system assessments.
Risk assessment under ICH Q3E employs a multi-dimensional approach that considers both the probability of extractables/leachables occurrence and the potential impact on product quality and patient safety. This assessment integrates factors such as contact time, temperature, pH, chemical compatibility, route of administration, patient population, and treatment duration. The framework explicitly acknowledges that risk varies significantly across different scenarios and requires tailored approaches rather than uniform requirements.
The risk control strategies outlined in ICH Q3E provide multiple pathways for managing identified risks, including material selection optimization, process parameter control, analytical monitoring, and specification limits. This flexibility enables pharmaceutical companies to develop cost-effective control strategies that are proportionate to the actual risks identified rather than applying maximum controls uniformly across all situations.
Lifecycle management ensures that E&L considerations remain integrated throughout product development, commercialization, and post-market surveillance. This includes provisions for managing material changes, process modifications, and the incorporation of new scientific knowledge as it becomes available. The lifecycle approach recognizes that E&L assessment is not a one-time activity but an ongoing process that must evolve with the product and available scientific understanding.
Safety Threshold Harmonization
ICH Q3E introduces a sophisticated threshold framework that harmonizes and extends the safety assessment principles developed through industry initiatives while addressing critical gaps in current approaches. The guideline establishes a risk-based threshold system that considers both mutagenic and non-mutagenic compounds while providing clear decision-making criteria for safety assessment.
For mutagenic compounds, ICH Q3E adopts a Threshold of Toxicological Concern (TTC) approach aligned with ICH M7 principles, establishing 1.5 μg/day as the default threshold for compounds with mutagenic potential. This represents harmonization with existing approaches while extending application to extractables and leachables that was previously addressed only through analogy or extrapolation.
For non-mutagenic compounds, the guideline introduces a tiered threshold system that considers route of administration, treatment duration, and patient population. The Safety Concern Threshold (SCT) varies based on these factors, with more conservative thresholds applied to high-risk scenarios such as parenteral administration or pediatric populations. This approach represents a significant advancement over current practice, which often applies uniform thresholds regardless of actual exposure scenarios or patient risk factors.
The Analytical Evaluation Threshold (AET) calculation methodology has been standardized and refined to provide consistent application across different analytical techniques and product configurations. The AET serves as the practical threshold for analytical identification and reporting, incorporating analytical uncertainty factors that ensure appropriate sensitivity for detecting compounds of potential safety concern.
The qualification threshold framework establishes clear decision points for when additional toxicological evaluation is required, reducing uncertainty and providing predictable pathways for safety assessment. Compounds below the SCT require no additional evaluation unless structural alerts are present, while compounds above the qualification threshold require comprehensive toxicological assessment using established methodologies.
Advanced Analytical Methodology Requirements
ICH Q3E establishes sophisticated analytical requirements that reflect advances in analytical chemistry and the increasing complexity of pharmaceutical products and manufacturing systems. The guideline requires fit-for-purpose analytical methods that are appropriately validated for their intended use, with particular emphasis on method capability to detect and quantify compounds at relevant safety thresholds.
The extraction study requirements have been standardized to ensure consistent generation of extractables profiles while allowing flexibility for product-specific optimization. The guideline establishes principles for solvent selection, extraction conditions, and extraction ratios that provide meaningful worst-case scenarios without introducing artifacts or irrelevant compounds. This standardization addresses a major source of variability in current practice, where different companies often use dramatically different extraction conditions that produce incomparable results.
Leachables assessment requirements emphasize the need for methods capable of detecting both known and unknown compounds in complex product matrices. The guideline recognizes the challenges associated with detecting low-level leachables in pharmaceutical formulations and provides guidance on method development strategies, including the use of placebo formulations, matrix subtraction approaches, and accelerated testing conditions that enhance detection capability.
The analytical uncertainty framework provides specific guidance on incorporating analytical variability into safety assessments, ensuring that measurement uncertainty does not compromise patient safety. This includes requirements for response factor databases, analytical uncertainty calculations, and the application of appropriate safety factors that account for analytical limitations.
Method validation requirements are tailored to the specific challenges of E&L analysis, including considerations for selectivity in complex matrices, detection limit requirements based on safety thresholds, and precision requirements that support reliable safety assessment. The guideline acknowledges that traditional pharmaceutical analytical validation approaches may not be directly applicable to E&L analysis and provides modified requirements that reflect the unique challenges of this application.
Material Science Integration and Innovation
ICH Q3E represents a significant advancement in the integration of material science principles into pharmaceutical quality systems. The guideline requires comprehensive material characterization that goes beyond simple compositional analysis to include understanding of manufacturing processes, potential degradation pathways, and interaction mechanisms that could lead to extractables formation.
The material selection guidance emphasizes proactive risk assessment during early development stages, enabling pharmaceutical companies to make informed material choices that minimize E&L risks rather than simply characterizing risks after materials have been selected. This approach aligns with Quality by Design principles and can significantly reduce development timelines and costs by avoiding late-stage material changes necessitated by unacceptable E&L profiles.
Single-use system assessment requirements reflect the increasing adoption of disposable manufacturing technologies in pharmaceutical production. The guideline provides specific frameworks for evaluating complex single-use assemblies that may contain multiple materials of construction and require additive risk assessment approaches. This addresses a critical gap in current guidance documents that were developed primarily for traditional reusable manufacturing equipment.
The guideline also addresses emerging materials and manufacturing technologies, including 3D-printed components, advanced polymer systems, and novel coating technologies. Provisions for evaluating innovative materials ensure that regulatory frameworks can accommodate technological advancement without compromising patient safety.
Comparison with Current Regulatory Frameworks
The transformative nature of ICH Q3E becomes evident when compared with existing regulatory approaches across different jurisdictions and application areas. The FDA’s 1999 Container Closure Systems guidance, while foundational, provides limited specific requirements and relies heavily on case-by-case assessment. This approach has led to significant variability in regulatory expectations and industry practice, creating uncertainty for both applicants and reviewers.
The EMA’s 2005 Plastic Immediate Packaging Materials guideline focuses specifically on plastic packaging materials and does not address the broader range of materials and applications covered by ICH Q3E. Additionally, the EMA guideline lacks specific safety thresholds, requiring product-specific risk assessment that can lead to inconsistent outcomes.
USP chapters <1663> and <1664> provide valuable technical guidance on extraction and leachables testing methodologies but do not establish safety thresholds or comprehensive risk assessment frameworks. These chapters serve as important technical references but require supplementation with safety assessment approaches from other sources.
The PQRI recommendations for orally inhaled and nasal drug products (OINDP) and parenteral and ophthalmic drug products (PODP) have provided industry-leading approaches to threshold-based safety assessment. However, these recommendations are limited to specific dosage forms and have not been formally adopted as regulatory requirements. ICH Q3E harmonizes and extends these approaches across all dosage forms while incorporating them into a formal regulatory framework.
Current European Pharmacopoeia requirements focus primarily on elemental extractables and do not address organic compounds comprehensively. The new EP chapter 2.4.35 on extractable elements represents an important advance but remains limited in scope compared to the comprehensive approach established by ICH Q3E.
ICH Q3E represents not merely an update or harmonization of existing approaches but a fundamental reconceptualization of E&L assessment that integrates the best elements of current practice while addressing critical gaps and inconsistencies.
Manufacturing Process Integration and Single-Use Systems
ICH Q3E places unprecedented emphasis on manufacturing process-related extractables and leachables, recognizing that modern pharmaceutical production increasingly relies on single-use systems, filters, tubing, and other disposable components that can contribute significantly to the overall E&L burden. This represents a major expansion from traditional container-closure system focus to encompass the entire manufacturing process.
The guideline establishes risk-based approaches for evaluating manufacturing equipment that consider factors such as contact time, process conditions, downstream processing steps, and the cumulative impact of multiple single-use components. This additive assessment approach acknowledges that even individually low-risk components can contribute to significant overall E&L levels when multiple components are used in series.
Single-use system assessment requirements address the complexity of modern bioprocessing equipment that may contain dozens of different materials of construction in a single assembly. The guideline provides frameworks for component-level assessment, assembly-level evaluation, and process-level integration that enable comprehensive risk assessment while maintaining practical feasibility.
The integration of manufacturing process E&L assessment with traditional container-closure system evaluation provides a holistic view of potential patient exposure that reflects the reality of modern pharmaceutical manufacturing. This comprehensive approach ensures that all sources of potential extractables and leachables are identified and appropriately controlled.
Biological Product Considerations and Specialized Applications
ICH Q3E provides specific considerations for biological products that reflect the unique challenges associated with protein stability, immunogenicity risk, and complex formulation requirements. Biological products often require specialized container-closure systems, delivery devices, and manufacturing processes that create distinct E&L challenges not adequately addressed by approaches developed for small molecule drugs.
The guideline addresses the potential for extractables and leachables to impact protein stability, aggregation, and biological activity through mechanisms that may not be captured by traditional chemical analytical approaches. This includes consideration of subvisible particle formation, protein adsorption, and catalytic degradation pathways that can be initiated by trace levels of extractables or leachables.
Immunogenicity considerations are explicitly addressed, recognizing that even very low levels of certain extractables or leachables could potentially trigger immune responses in sensitive patient populations. The guideline provides frameworks for assessing immunogenic risk that consider both the chemical nature of potential leachables and the clinical context of the biological product.
Cell and gene therapy applications receive special attention due to their unique manufacturing requirements, complex delivery systems, and often highly vulnerable patient populations. The guideline provides tailored approaches for these emerging therapeutic modalities that reflect their distinct risk profiles and manufacturing challenges.
Analytical Method Development and Validation Evolution
The analytical requirements established by ICH Q3E requires method capabilities that extend beyond traditional pharmaceutical analysis to encompass broad-spectrum unknown identification and quantification in complex matrices. This creates both challenges and opportunities for analytical laboratories and method development organizations.
Method development requirements emphasize systematic approaches to achieving required detection limits while maintaining selectivity in complex product matrices. The guideline provides specific guidance on extraction efficiency verification, matrix effect assessment, and the development of appropriate reference standards for quantification. These requirements ensure that analytical methods provide reliable data for safety assessment while maintaining practical feasibility.
Validation requirements are tailored to the unique challenges of E&L analysis, including considerations for compound identification confidence, quantification accuracy across diverse chemical structures, and method robustness across different product matrices. The guideline acknowledges that traditional pharmaceutical validation approaches may not be appropriate for E&L methods and provides modified requirements that reflect the specific challenges of this application.
The requirement for analytical uncertainty assessment and incorporation into safety evaluation represents a significant advancement in analytical quality assurance. Methods must not only provide accurate results but must also provide reliable estimates of measurement uncertainty that can be incorporated into risk assessment calculations.
Global Implementation Challenges and Opportunities
The implementation of ICH Q3E will require significant changes in pharmaceutical company practices, analytical capabilities, and regulatory review processes across all ICH regions. The comprehensive nature of the guideline means that virtually all pharmaceutical products will be impacted to some degree, creating both implementation challenges and opportunities for improved efficiency.
Training requirements will be substantial, as the guideline requires expertise in materials science, analytical chemistry, toxicology, and risk assessment that may not currently exist within all pharmaceutical organizations. The development of specialized E&L expertise will become increasingly important as companies seek to implement the guideline effectively.
Analytical infrastructure requirements may necessitate significant investments in instrumentation, method development capabilities, and reference standards. Smaller pharmaceutical companies may need to partner with specialized contract laboratories to access the required analytical capabilities.
Regulatory review processes will need to evolve to accommodate the risk-based approaches and comprehensive documentation requirements established by the guideline. Regulatory authorities will need to develop expertise in E&L assessment and establish consistent review practices across different therapeutic areas and product types.
The opportunities created by ICH Q3E implementation include improved regulatory predictability, reduced development timelines through early risk identification, and enhanced patient safety through more comprehensive E&L assessment. The harmonized approach should reduce the regulatory burden associated with multi-regional submissions while improving the overall quality of E&L assessments.
Future Evolution and Emerging Technologies
ICH Q3E has been designed with sufficient flexibility to accommodate emerging technologies and evolving scientific understanding. The risk-based framework can be adapted to new materials, manufacturing processes, and delivery systems as they are developed and implemented.
The guideline’s emphasis on scientific principles rather than prescriptive requirements enables adaptation to technological advances such as continuous manufacturing, advanced drug delivery systems, and personalized medicine approaches. This forward-looking design ensures that the guideline will remain relevant as pharmaceutical technology continues to evolve.
Provisions for incorporating new toxicological data and analytical methodologies ensure that the guideline can evolve with advancing scientific understanding. The lifecycle management approach enables updates and refinements based on accumulated experience and emerging scientific knowledge.
The integration with other ICH guidelines creates synergies that will facilitate future development of related guidance documents and ensure consistency across the broader ICH framework. This systematic approach to guideline development enhances the overall effectiveness of international pharmaceutical regulation.
Economic Impact and Industry Transformation
The implementation of ICH Q3E will have significant economic implications for the pharmaceutical industry, both in terms of implementation costs and long-term benefits. Initial implementation will require substantial investments in analytical capabilities, personnel training, and process modifications. However, the long-term benefits of harmonized requirements, improved regulatory predictability, and enhanced product quality are expected to provide significant value.
The harmonized approach should reduce the overall cost of global product development by eliminating duplicate testing requirements and reducing regulatory review timelines. Companies will be able to develop single global E&L strategies rather than maintaining multiple region-specific approaches.
Contract research organizations and analytical service providers will need to develop specialized capabilities to support pharmaceutical company implementation efforts. This will create new market opportunities while requiring significant investments in infrastructure and expertise.
The enhanced focus on risk-based assessment should enable more efficient allocation of resources to genuine safety concerns while reducing unnecessary testing and evaluation activities. This optimization of effort should improve overall industry efficiency while enhancing patient safety.
Patient Safety Enhancement and Risk Mitigation
The ultimate objective of ICH Q3E is enhanced patient safety through more comprehensive and scientifically rigorous assessment of extractables and leachables risks. The guideline achieves this objective through multiple mechanisms that address current gaps and limitations in E&L assessment practice.
The comprehensive material assessment requirements ensure that all potential sources of extractables and leachables are identified and evaluated. This includes not only traditional packaging materials but also manufacturing equipment, delivery device components, and any other materials that could contribute to patient exposure.
The harmonized safety threshold framework provides consistent and scientifically defensible criteria for safety assessment across all product types and administration routes. This eliminates the variability and uncertainty that can arise from inconsistent threshold application in current practice.
The risk-based approach enables appropriate allocation of assessment effort to genuine safety concerns while avoiding unnecessary evaluation of trivial risks. This optimization ensures that resources are focused on protecting patient safety rather than simply meeting regulatory requirements.
The lifecycle management requirements ensure that E&L considerations remain current throughout product development and commercialization. This ongoing attention to E&L issues helps identify and address emerging risks that might not be apparent during initial assessment.
Conclusion
ICH Q3E represents far more than an incremental improvement in extractables and leachables guidance; it establishes a new paradigm for pharmaceutical quality assurance that integrates materials science, analytical chemistry, toxicology, and risk management into a comprehensive framework that reflects the complexity of modern pharmaceutical development and manufacturing.
The guideline’s emphasis on scientific principles over prescriptive requirements creates a flexible framework that can accommodate the diverse and evolving landscape of pharmaceutical products while maintaining rigorous safety standards. This approach represents a significant maturation of regulatory science that moves beyond one-size-fits-all requirements to embrace risk-based, scientifically defensible assessment approaches.
The global harmonization achieved through ICH Q3E addresses one of the most significant challenges facing the pharmaceutical industry by providing consistent requirements and expectations across all major regulatory jurisdictions. This harmonization will facilitate more efficient global product development while enhancing patient safety through improved assessment practices.
The comprehensive scope of ICH Q3E ensures that extractables and leachables assessment evolves from a specialized concern for specific dosage forms to an integral component of pharmaceutical quality assurance across all products and therapeutic modalities. This integration reflects the reality that E&L considerations impact virtually all pharmaceutical products and must be systematically addressed throughout development and commercialization.
As the pharmaceutical industry prepares for ICH Q3E implementation, the focus must be on building the scientific expertise, analytical capabilities, and quality systems necessary to realize the guideline’s potential for enhancing patient safety while improving development efficiency. The successful implementation of ICH Q3E will mark a new era in pharmaceutical quality assurance that better serves patients, regulators, and the pharmaceutical industry through more rigorous, consistent, and scientifically defensible approaches to extractables and leachables assessment.
The transformation initiated by ICH Q3E extends beyond technical requirements to encompass fundamental changes in how pharmaceutical companies approach material selection, process design, analytical strategy, and risk management. This holistic transformation will ultimately deliver safer, higher-quality pharmaceutical products to patients worldwide while establishing a more efficient and predictable regulatory environment that facilitates innovation and global access to medicines.
I have a few concerns about George Tidmarsh’s recent appointment as director of the FDA’s Center for Drug Evaluation and Research (CDER) which fits into wider concerns about the current administration. As usual in this adminstration, this boils down to a tendency to fringe medicine and vaccine denial adjacent thinking.
Association with “fringe” medical publishing: Tidmarsh contributed to the Journal of the Academy of Public Health, which Bloomberg and other outlets have described as a “fringe medical journal” connected to a conservative nonprofit.
Criticism of COVID-19 public health policy: Tidmarsh has openly criticized the government’s handling of the COVID-19 pandemic. On the “Derate the Hate” podcast, he lamented what he saw as political polarization and lack of “academic freedom” in pandemic-era policy discussions, and suggested openness to the theory of a lab origin for the coronavirus.
I also find a degree of irony in Tidmarsh’s leadership roles in several biotech and pharmaceutical companies—including as founder and CEO of Horizon Therapeutics and Threshold Pharmaceuticals. RFKJr, and others have spent a lot of time criticizing the revolving door between industry and government regulation. And here we have a great example of that revolving door.
In any other administration, Tidmarsh would be concerning due to his connections to fringe science. In this administration he is another worrisome personnel decision given authority.