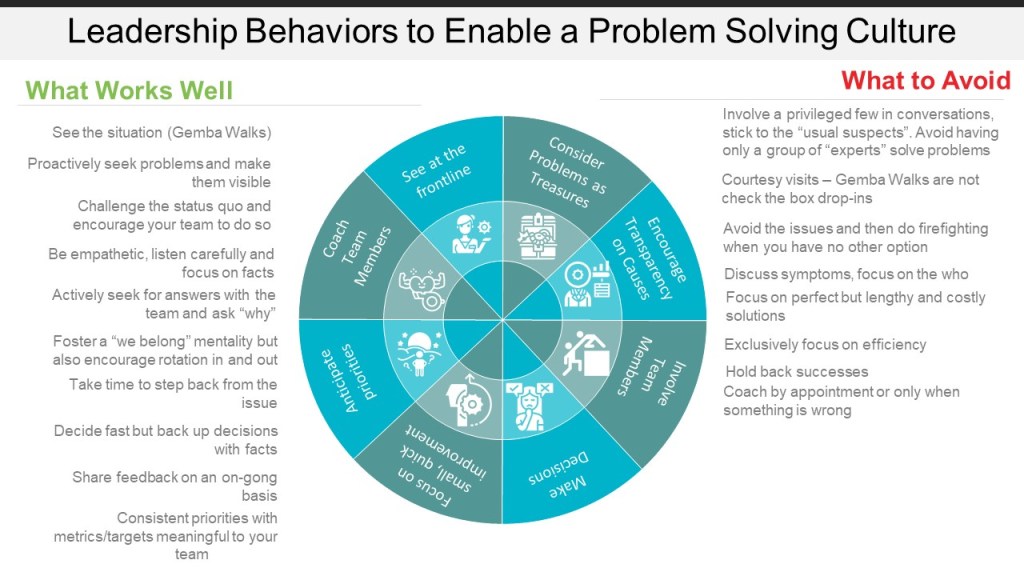
Leadership is a critical element of a problem solving culture and rightly is emphasized in frameworks like the Baldridge or standards like ISO 9001:2015. Leadership is best looked at as the process for determining a possible future state that does not yet exist. As we strive to build excellence we need a passion for this work and to believe it to be truly important. Sharing that enthusiasm is motivating for all people involved and is a way to leverage greater success.
Good leaders encourage behaviors to maintain and improve quality by means of sound decision-making and risk-based thinking.
All of these leadership behaviors stem from four building blocks:
Anticipation of likely future needs, trends and options.
Let’s be honest – slides and presentations from quality professionals tend to be text heavy and graphic poor. I’m no expert here, but I have settled on a few subscriptions that help me produce fair to middling presentations and graphics.
SlideModel, SlideGeeks, SlideTeam – You probably don’t want all three (or one of the other competitors) but have a subscription to just one of these have saved my sanity more times than I can count.
NounProject – Oh how I love the icons this organization makes available. I use them everywhere! Presentations, procedures, technical systems. Great price structure, decent licensing. Now with a decent photo library too. Someday I will organize one of their Iconathons for developing a good set of icons around quality principles and tools.
Photolibrary – So many free and low priced ones out there. I don’t use photos nearly enough but I keep up a low level shutterstock subscription and use my monthly quota.
My goal this year is to use more graphics in my blog. Well actually my goal is to post more this year, 2020 was kind of a wash.
Improvement is a process and sometimes it can feel like it is a one-step-forward-two-steps-back sort of shuffle. And just like any dance, knowing the steps to avoid can be critical. Here are some important ones to consider. In many ways they can be considered an onion, we systematically can address a problem layer and then work our way to the next.
Human-error-as-cause
The vague, ambiguous and poorly defined bucket concept called human error is just a mess. Human error is never the root cause; it is a category, an output that needs to be understood. Why did the human error occur? Was it because the technology was difficult to use or that the procedure was confusing? Those answers are things that are “actionable”—you can address them with a corrective action.
The only action you can take when you say “human error” is to get rid of the people. As an explanation the concept it widely misused and abused.
Human error has been a focus for a long time, and many companies have been building programmatic approaches to avoiding this pitfall. But we still have others to grapple with.
Causal Chains
We like to build our domino cascades that imply a linear ordering of cause-and-effect – look no further than the ubiquitous presence of the 5-Whys. Causal chains force people to think of complex systems by reducing them when we often need to grapple with systems for their tendency towards non-linearity, temporariness of influence, and emergence.
This is where taking risk into consideration and having robust problem-solving with adaptive techniques is critical. Approach everything like a simple problem and nothing will ever get fixed. Similarly, if every problem is considered to need a full-on approach you are paralyzed. As we mature we need to have the mindset of types of problems and the ability to easily differentiate and move between them.
Root cause(s)
We remove human error, stop overly relying on causal chains – the next layer of the onion is to take a hard look at the concept of a root cause. The idea of a root cause “that, if removed, prevents recurrence” is pretty nonsensical. Novice practitioners of root cause analysis usually go right to the problem when they ask “How do I know I reached the root cause.” To which the oft-used stopping point “that management can control” is quite frankly fairly absurd. The concept encourages the idea of a single root cause, ignoring multiple, jointly necessary, contributory causes let alone causal loops, emergent, synergistic or holistic effects. The idea of a root cause is just an efficiency-thoroughness trade-off, and we are better off understanding that and applying risk thinking to deciding between efficiency and resource constraints.
In conclusion
Our problem solving needs to strive to drive out monolithic explanations, which act as proxies for real understanding, in the form of big ideas wrapped in simple labels. The labels are ill-defined and come in and out of fashion – poor/lack of quality culture, lack of process, human error – that tend to give some reassurance and allow the problem to be passed on and ‘managed’, for instance via training or “transformations”. And yes, maybe there is some irony in that I tend to think of the problems of problem solving in light of these ways of problem solving.
Last night speaking at the DFW Audit SIG one of the topics I wished I had gone a little deeper on were controls, and how to gauge their strength.
As I am preparing to interview candidates for a records management position, I thought I would flesh out controls specific to the storage of and access to completed or archived paper records, such as forms, as an example.
These controls are applied at the record or system level and are meant to prevent a potential data integrity issue from occurring.
Generation and Reconciliation of Documents
Data Criticality
High
Medium
Low
Unique identifier
For each record
No
No
Who performs controlled issuance
Individuals authorized by quality unit from designated unit (limited, centralized)
Individuals authorized by quality unit from (limited, decentralized)
Anyone (unlimited, decrentalized), often user of record
Reconciliation
Full reconciliation of record and pages based on unique identifier
Full reconciliation of records and pages based on quantity issued
No reconciliation
Controlled print
Yes
Yes
No
Bulk printing
No
Yes, by controlled process
Yes
Destruction of blank forms
Performed by issuing unit, quality oversight required (High level of evidence)
Performed by the operating or issuing unit, quality unit oversight required
Performed by the individual, quality unit oversight required (periodic walk throughs, self-inspections and audits)
Storage and Access to completed and archived paper records
Data Criticality
High
Medium
Low
Where Stored
Climate-controlled room
Climate-controlled room
Office retention location
How Removed & Returned
Limited conditions for removal (e.g. regulatory inspections) method of recording the removal and return of the record(e.g. archive management system, logbook). Most use of documents either in controlled reading area or by scans.
Method of recording the removal and return of the record(e.g., archive management system, logbook).
Method (e.g. logbook) recording of documents checked-in/checked-out
Access Control
Card key access with entry and exit documented.
Card key access with entry and exit documented.
Limited key access
Periodic User Access Review
Annually
Annually
Every 2 years
There are also the need to consider controls for paper to electronic, electronic to paper and my favorite beast, the true copy.
For paper records a true copy of a picture of the original that keeps everything – a scan. The regulations state that you can get rid of the paper if you have a true copy. Many things called a true copy are probably not a true copy, to ensure an accurate true copy add two more controls.
Data Criticality
High
Medium
Low
Review requirements
Documented review by second person from the quality unit for legibility, accuracy, and completeness
Documented review by second person (not necessarily from the quality unit) for legibility, accuracy, and completeness
Documented verification by person performing the scan for legibility, accuracy, and completeness
Discard of original allowed
Yes, as defined by quality unit oversight, unless there is a seal, watermark, or other identifier that can’t be accurately reproduced electronically.
Yes, performed by the operating unit, unless there is a seal, watermark, or other identifier that can’t be accurately reproduced electronically. Quality unit oversight required
Yes, individual can discard original Quality unit oversight required
The Barr decision, issued 28 years ago, explains how to deal with OOS results. The FDA followed up with a guidance in 2006 “Guidance for Industry Investigating Out-of-Specification (OOS) Test Results for Pharmaceutical Production.” Companies have no excuse for continued failure here, and yet as we see with Allay (and so many others) failures in investigation of out-of-specifications continues to be a major concern. Yet nothing we see is not covered in the Barr decision.
If you a pharmaceutical GMP professional these three documents should be ones you are more than ready to explain against your quality system.