In the continual saga of companies making fundamental GMP mistakes, Gilead has recalled two lots of its coronavirus treatment drug Remdesivir because of the “presence of glass particulates.”
If only there existed international standards on visual inspection and there were a solid set of best practices on lyophilization.
Oh, wait there are.
But then Gilead has a multi-year track record in deficiencies in their testing and manufacturing processes. In all fairness, they are contracting manufacturing to Pfizer’s McPherson site…..oh wait that site got an FDA 483 in 2018 specifying significant violations of good manufacturing practices, such as an inadequate investigation into the detected presence of cardboard in vial samples.
We deserve better manufacturers. Companies need to take the quality of their products seriously. We are always improving or we are always one step away from the sort of press Gilead gets.
All three are right on the nose, and I’ve posted a bunch on the topics. Definitely go and read the post.
What I want to delve deeper into is Stephanie’s point that “Deviation systems should also be built to triage events into risk-based categories with sufficient time allocated to each category to drive risk-based investigations and focus the most time and effort on the highest risk and most complex events.”
That is an accurate breakdown, and exactly what regulators are asking for. However, I think the implementation of risk-based categories can sometimes lead to confusion, and we can spend some time unpacking the concept.
Risk is the possible effect of uncertainty. Risk is often described in terms of risk sources, potential events, their consequences, and their likelihoods (where we get likelihoodXseverity from).
But there are a lot of types of uncertainty, IEC31010 “Risk management – risk management techniques” lists the following examples:
uncertainty as to the truth of assumptions, including presumptions about how people or systems might behave
variability in the parameters on which a decision is to be based
uncertainty in the validity or accuracy of models which have been established to make predictions about the future
events (including changes in circumstances or conditions) whose occurrence, character or consequences are uncertain
uncertainty associated with disruptive events
the uncertain outcomes of systemic issues, such as shortages of competent staff, that can have wide ranging impacts which cannot be clearly defined lack of knowledge which arises when uncertainty is recognized but not fully understood
unpredictability
uncertainty arising from the limitations of the human mind, for example in understanding complex data, predicting situations with long-term consequences or making bias-free judgments.
Most of these are only, at best, obliquely relevant to risk categorizing deviations.
So it is important to first build the risk categories on consequences. At the end of the day these are the consequence that matter in the pharmaceutical/medical device world:
harm to the safety, rights, or well-being of patients, subjects or participants (human or non-human)
compromised data integrity so that confidence in the results, outcome, or decision dependent on the data is impacted
These are some pretty hefty areas and really hard for the average user to get their minds around. This is why building good requirements, and understanding how systems work is so critical. Building breadcrumbs in our procedures to let folks know what deviations are in what category is a good best practice.
There is nothing wrong with recognizing that different areas have different decision trees. Harm to safety in GMP can mean different things than safety in a GLP study.
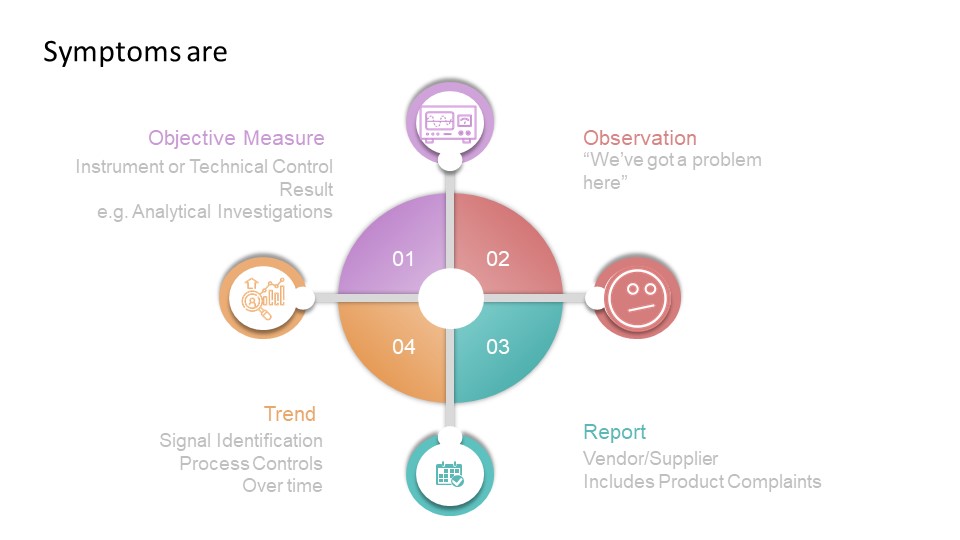
The second place I’ve seen this go wrong has to do with likelihood, and folks getting symptom confused with problem confused with cause.
bridge with a gap
All deviations are with a situation that is different in some way from expected results. Deviations start with the symptom, and through analysis end up with a root cause. So when building your decision-tree, ensure it looks at symptoms and how the symptom is observed. That is surprisingly hard to do, which is why a lot of deviation criticality scales tend to focus only on severity.
The quality profession in the pharmaceutical industry is wider than the overseeing regulations from health authorities. The GXPs are truly a starting point, not an ending point which is why we often use that little “c” for “current.”
The GXPs (and the regulations behind them) serve an important purpose. But they are the start of excellence and not the end.
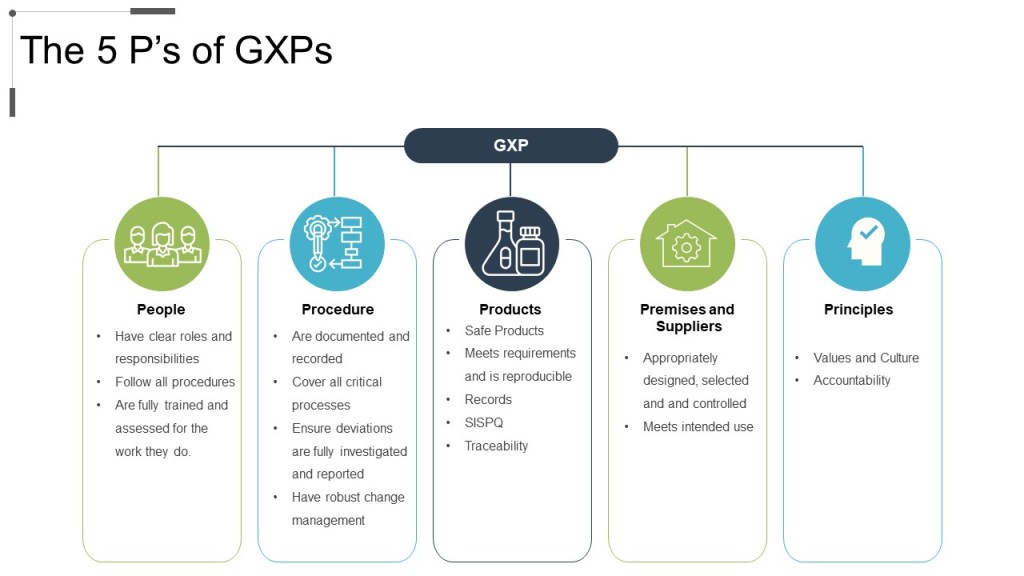
The GXPs are an outline. When we start with these requirements and then fill in the details we build a robust and beautiful engine for quality.
The 5Ps of GXPs: People, Procedure, Product, Premise, and Principles.
This is often why we talk about compliance being the start of quality, and not the end.
ERC The Netherlands B.V. received thirteen deficiencies from a recent inspection, one of which was classified as a critical deficiency.
These were mainly related to five main components:
Quality and safety of starting materials. Inspection of chemicals and consumables is insufficient.
The quality and safety of the final product is not guaranteed. The product is not sufficiently defined and characterized.
The effectiveness of a gama irradiation step, and therefore the safety of the product, is not guaranteed.
The change for the transition from Contractor 1 to Contractor 2 for gamma irradiation of cells has not been carried out as referred to in the GMP for ATMPs.
Prevention of (cross) contamination is not sufficiently guaranteed.
The environmental monitoring program and personnel monitoring are inadequate.
Reviewing this together with Emergent’s 483 (and resulting actions) starts to define a set of concerns in the ATMP world.
Lilly has had several decades of “promising to address GMP issues.” Are these signs of not addressing cultural issues? Of the balkanization of fixes? Of the infamous pendulum swing? I have no insight, but as an individual who was involved in the work of consent decree remediation at another company, I certainly have lots of questions about what is up at Lilly.