The allure of shiny new tools in quality management is undeniable. Like magpies drawn to glittering objects, professionals often collect methodologies and technologies without a cohesive strategy. This “magpie syndrome” creates fragmented systems—FMEA here, 5S there, Six Sigma sprinkled in—that resemble disjointed toolkits rather than coherent ecosystems. The result? Confusion, wasted resources, and quality systems that look robust on paper but crumble under scrutiny. The antidote lies in reimagining quality systems not as static machines but as living organizations that evolve, adapt, and thrive.
The Shift from Machine Logic to Organic Design
Traditional quality systems mirror 20th-century industrial thinking: rigid hierarchies, linear processes, and documents that gather dust. These systems treat organizations as predictable machines, relying on policies to command and procedures to control. Yet living systems—forests, coral reefs, cities—operate differently. They self-organize around shared purpose, adapt through feedback, and balance structure with spontaneity. Deming foresaw this shift. His System of Profound Knowledge—emphasizing psychology, variation, and systems thinking—aligns with principles of living systems: coherence without control, stability with flexibility.
At the heart of this transformation is the recognition that quality emerges not from compliance checklists but from the invisible architecture of relationships, values, and purpose. Consider how a forest ecosystem thrives: trees communicate through fungal networks, species coexist through symbiotic relationships, and resilience comes from diversity, not uniformity. Similarly, effective quality systems depend on interconnected elements working in harmony, guided by a shared “DNA” of purpose.
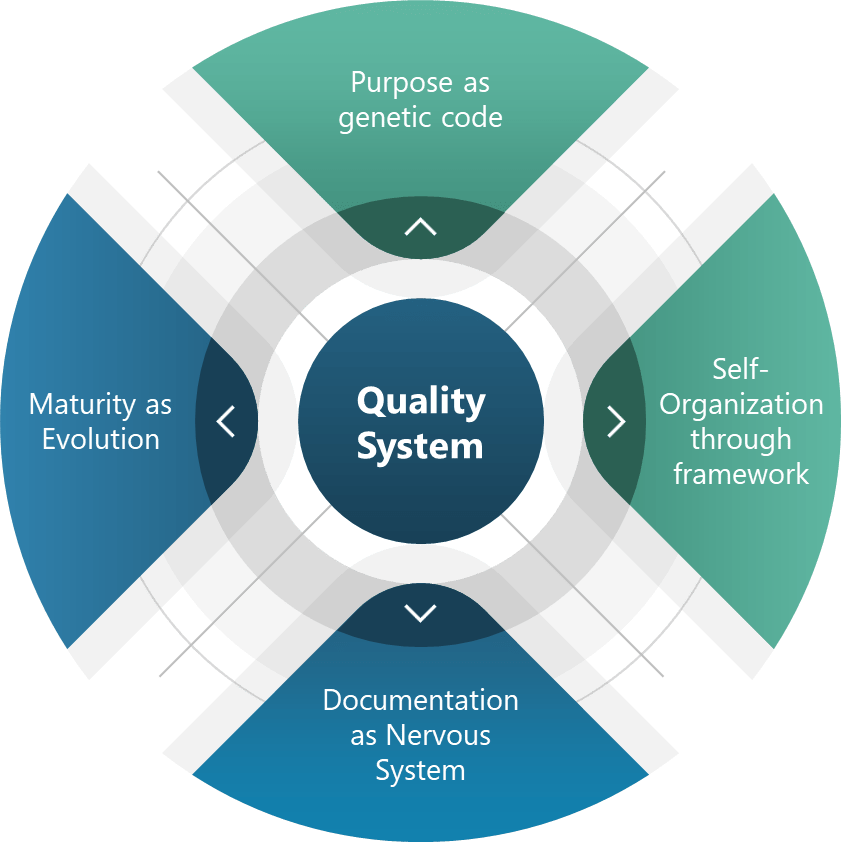
The Four Pillars of Living Quality Systems
Purpose as Genetic Code Every living system has inherent telos—an aim that guides adaptation. For quality systems, this translates to policies that act as genetic non-negotiables. For pharmaceuticals and medical devices this is “patient safety above all.”. This “DNA” allowed teams to innovate while maintaining adherence to core requirements, much like genes express differently across environments without compromising core traits.
Self-Organization Through Frameworks Complex systems achieve order through frameworks as guiding principles. Coherence emerges from shared intent. Deming’s PDSA cycles and emphasis on psychological safety create similar conditions for self-organization.
Documentation as a Nervous System The enhanced document pyramid—policies, programs, procedures, work instructions, records—acts as an organizational nervous system. Adding a “program” level between policies and procedures bridges the gap between intent and action and can transform static documents into dynamic feedback loops.
Maturity as Evolution Living systems evolve through natural selection. Maturity models serve as evolutionary markers:
Ad-hoc (Primordial): Tools collected like random mutations.
Sustainability: Planning for decade-long impacts, not quarterly audits.
Elegance: Simplifying until it hurts, then relaxing slightly.
Coordination: Cross-pollinating across the organization
Convenience: Making compliance easier than non-compliance.
These principles operationalize Deming’s wisdom. Driving out fear (Point 8) fosters psychological safety, while breaking down barriers (Point 9) enables cross-functional symbiosis.
The Quality Professional’s New Role: Gardener, Not Auditor
Quality professionals must embrace a transformative shift in their roles. Instead of functioning as traditional enforcers or document controllers, we are now called to act as stewards of living systems. This evolution requires a mindset change from one of rigid oversight to one of nurturing growth and adaptability. The modern quality professional takes on new identities such as coach, data ecologist, and systems immunologist—roles that emphasize collaboration, learning, and resilience.
To thrive in this new capacity, practical steps must be taken. First, it is essential to prune toxic practices by eliminating fear-driven reporting mechanisms and redundant tools that stifle innovation and transparency. Quality professionals should focus on fostering trust and streamlining processes to create healthier organizational ecosystems. Next, they must plant feedback loops by embedding continuous learning into daily workflows. For instance, incorporating post-meeting retrospectives can help teams reflect on successes and challenges, ensuring ongoing improvement. Lastly, cross-pollination is key to cultivating diverse perspectives and skills. Rotating staff between quality assurance, operations, and research and development encourages knowledge sharing and breaks down silos, ultimately leading to more integrated and innovative solutions.
By adopting this gardener-like approach, quality professionals can nurture the growth of resilient systems that are better equipped to adapt to change and complexity. This shift not only enhances organizational performance but also fosters a culture of continuous improvement and collaboration.
Thriving, Not Just Surviving
Quality systems that mimic life—not machinery—turn crises into growth opportunities. As Deming noted, “Learning is not compulsory… neither is survival.” By embracing living system principles, we create environments where survival is the floor, and excellence is the emergent reward.
Start small: Audit one process using living system criteria. Replace one control mechanism with a self-organizing principle. Share learnings across your organizational “species.” The future of quality isn’t in thicker binders—it’s in cultivating systems that breathe, adapt, and evolve.
The International Conference on Harmonization (ICH) was established to harmonize the technical requirements for pharmaceutical product registration across Europe, Japan, and the United States. ICH Q10, finalized in June 2008, emerged from this initiative as a guideline for a comprehensive Pharmaceutical Quality System (PQS) applicable throughout the product lifecycle. It was adopted by the FDA in April 2009, following its implementation by the European Commission in July 2008.
ICH Q10 aims to provide a model for pharmaceutical manufacturers to develop and maintain effective quality management systems. The guideline emphasizes a lifecycle approach, integrating quality management principles from ISO standards and regional GMP requirements. The primary objectives of ICH Q10 include:
Ensuring consistent product quality that meets customer and regulatory requirements.
Establishing effective monitoring and control systems for process performance and product quality.
Promoting continual improvement and innovation throughout the product lifecycle.
The guideline outlines the key elements of management responsibilities, Corrective and Preventive Action (CAPA) , process performance and product quality monitoring, change management, and management review. ICH Q10 is usually considered part of the “Quality Trio” with ICH Q8 and Q9. Quality by design is only possible through proper risk management and a robust quality system.
FDA Guidance for Industry on Quality Systems Approach to Pharmaceutical CGMP Regulation
The FDA developed guidance on implementing modern quality systems and risk management practices to align with the CGMP (Current Good Manufacturing Practice) requirements outlined in parts 210 and 211 of the FDA regulations. These regulations govern the manufacturing of human and veterinary drugs, including biological products. Published in 2006, this guidance should be viewed as part of a continuum of thought with ICH Q10 and not as an earlier draft.
This guidance aims to assist manufacturers in meeting cGMP requirements by adopting a comprehensive quality systems model. It emphasizes the integration of quality systems with regulatory requirements to ensure full compliance without imposing new expectations on manufacturers. Key aspects of the guidance include:
Highlighting the consistency of the quality systems model with cGMP regulations.
Encouraging the use of risk management and quality systems to enhance compliance and product quality.
Providing a framework for manufacturers to gain control over their manufacturing processes.
Six-System Inspection Model
The FDA’s Six-System Inspection Model is a framework introduced in this guidance to ensure compliance with current Good Manufacturing Practice (CGMP) regulations in the pharmaceutical industry. This model helps FDA inspectors evaluate the robustness of a company’s quality management system by focusing on six key subsystems.
I am a huge fan of the six subsystem approach. Basically we have here the organization of the quality manual, a guide to what standards you need to write in a bigger company, and a franework for understanding the cGMPs as a whole (great for education purposes).
Here’s a detailed explanation of each subsystem:
1. Quality System
Role: Acts as the central hub for all other systems, ensuring overall quality management.
Focus: Management responsibilities, internal audits, CAPA (Corrective and Preventive Actions), and continuous improvement.
Importance: Ensures that all other systems are effectively integrated and managed to maintain product quality and regulatory compliance.
2. Facilities and Equipment System
Role: Ensures that facilities and equipment are suitable for their intended use and maintained properly.
Focus: Design, maintenance, cleaning, and calibration of facilities and equipment.
Importance: Prevents contamination and ensures consistent manufacturing conditions.
3. Materials System
Role: Manages the control of raw materials, components, and packaging materials.
Focus: Supplier qualification, receipt, storage, inventory control, and testing of materials.
Importance: Ensures that only high-quality materials are used in the manufacturing process, reducing the risk of product defects.
4. Production System
Role: Oversees the actual manufacturing processes.
Focus: Process controls, batch records, in-process controls, and validation.
Importance: Ensures that products are manufactured consistently and meet predefined quality criteria.
5. Packaging and Labeling System
Role: Manages the packaging and labeling processes to ensure correct and compliant product presentation.
Focus: Label control, packaging operations, and labeling verification.
Importance: Prevents mix-ups and ensures that products are correctly identified and used.
6. Laboratory Controls System
Role: Ensures the reliability of laboratory testing and data integrity.
Focus: Sampling, testing, analytical method validation, and laboratory records.
Importance: Verifies that products meet quality specifications before release.
Integration and Interdependence
Quality System as the Fulcrum: The quality system is the central element that integrates all other subsystems. It ensures that each subsystem functions correctly and is aligned with overall quality objectives.
State of Control: The primary goal of the six-system inspection model is to ensure that each subsystem is in a state of control, meaning it operates within predefined limits and consistently produces the desired outcomes.
The Six-System Inspection Model provides a structured approach for FDA inspectors to assess the compliance and effectiveness of a pharmaceutical company’s quality management system. By focusing on these six subsystems, the FDA ensures that all aspects of manufacturing, from raw materials to final product testing, are adequately controlled and managed to maintain high standards of product quality and safety.
A Complementary and Holistic Approach
Both ICH Q10 and the FDA’s guidance on quality systems approach aim to enhance the quality and safety of pharmaceutical products through robust quality management systems. ICH Q10 provides a harmonized model applicable across the product lifecycle, while the FDA guidance focuses on integrating quality systems with existing CGMP regulations. Together, they support the pharmaceutical industry in achieving consistent product quality and regulatory compliance.
Aspect
ICH Q10
FDA Guidance on CGMP
ISO 13485 and 21 CFR 820
ISO 9000
Purpose and Scope
Comprehensive model for pharmaceutical quality systems across the product lifecycle.
Quality systems approach to ensure CGMP compliance in pharmaceuticals.
Quality management system for medical devices, incorporating ISO 13485 and regulatory requirements of 21 CFR 820.
Fundamentals and vocabulary for quality management systems applicable to any industry.
Industry Focus
Specifically for the pharmaceutical industry.
Specifically for the pharmaceutical industry.
Specifically for the medical device industry.
Applicable to any industry.
Key Elements
Management responsibilities, CAPA, process performance, change management, management review.
Management responsibilities, quality systems, process validation, continuous improvement.
Quality management principles, terms, and definitions.
Regulatory Focus
Strong emphasis on regulatory compliance and lifecycle management.
Strong emphasis on regulatory compliance with CGMP.
Incorporates regulatory requirements specific to medical devices (21 CFR 820).
Does not directly address regulatory compliance.
Flexibility
Flexible, adaptable to specific product and process needs.
More prescriptive with specific compliance requirements.
Harmonized with international standards but includes specific regulatory requirements.
Provides a broad framework for customization.
Management Involvement
Emphasizes management’s role in quality and regulatory compliance.
Emphasizes management’s role in quality and CGMP integration.
Emphasizes management’s role in quality and risk-based decision making.
Emphasizes management’s role in quality and customer satisfaction.
Implementation
Tailored to pharmaceutical manufacturing, integrating quality management principles.
Mandates oversight and controls over drug manufacturing processes.
Requires a quality manual and specific documentation practices; aligned with international standards.
Requires customization to specific industry needs.
These two documents were developed at the same time and represents the thinking twenty years ago in laying down an approach that still matters today. I usually regard the six system approach as a deepening and defining of what Q10 means by process performance and product quality monitoring.
What is the current agency thinking?
The FDA and other revulatory agencies haven’t stopped their thinking in 2008. Sixteen years later we see the continued push for quality culture and quality maturity. The FDA continues to make this a top priority, as we’ve been seeing in their annual drug shortage reports to Congress. There are a few themes we continue to see driven home.
The Patient is the Customer
Quality management must be customer-focused, ensuring that all processes and materials meet their intended use. Senior management’s commitment is crucial for a strong QMS, which emphasizes proactive quality assurance over reactive quality control. Robust supplier relationships and oversight programs are essential to manage variability in materials and processes.
This application of a core priciple in ISO 9000 may seem to basic to some, but I think it is central to a lot of messaging and should never be taken for granted.
Benefits of Better Quality Performance
A continued focus that a quality-focused culture leads to:
Early problem detection
Enhanced process stability and productivity
Fewer major deviations and failures
Efficient QA release of batches
Reduced customer complaints and returns
Protection of brand and competitiveness
Management Oversight of Drug Quality
Management must address sources of variability, including people, materials, methods, measurements, machines, and environment. Risk management should be dynamic and ongoing, facilitating continual learning and improvement.
Corrective Action and Preventive Action (CAPA)
A structured approach to investigating complaints, product rejections, nonconformances, recalls, deviations, audits, regulatory inspections, and trends is essential. CAPA should determine root causes and implement corrective actions.
Change Management
Timely and effective change management ensures corrections and improvements are undertaken efficiently. This includes implementing product quality improvements, process improvements, variability reduction, innovations, and pharmaceutical quality system enhancements.
Management Review
Management is responsible for quality policy, QMS effectiveness, internal communications, resource management, and supply chain oversight. This includes ensuring the quality of incoming materials and outsourced activities.
Quality Culture Driven by Top Management
A strong corporate quality culture is driven by daily decisions and executive oversight. Sustainable compliance requires aiming for high standards rather than just meeting minimum requirements. Quality management maturity involves proactive and preventive actions, iterative learning, and leveraging modern technologies.
Facility Lifecycle
Senior management must ensure the suitability of operational design, control, and maintenance. This includes addressing infrastructure reliability, appropriateness for new product demands, and mitigating equipment/facility degradation.
Risk Management in Manufacturing
Human factors and manual interventions pose significant risks in pharmaceutical manufacturing. Automation and separation technologies can mitigate these risks, but many facilities still rely on manually intensive processes. Leveraging new technologies and practices is a huge opportunity.
This approach is reflected in the FDA’s Quality Management Maturity (QMM), which promotes advanced quality management practices within drug manufacturing establishments.
Goals of the QMM Program
Foster a Strong Quality Culture Mindset: Encourage establishments to integrate quality deeply into their organizational culture.
Recognize Advanced Quality Management Practices: Acknowledge and reward establishments that go beyond basic CGMP (Current Good Manufacturing Practices) requirements.
Identify Growth Opportunities: Provide suggestions for enhancing quality management practices.
Minimize Risks to Product Availability: Ensure a reliable market supply by reducing quality-related failures and maintaining performance during supply chain disruptions.
Key Components of the QMM Program
Management Commitment to Quality: Leadership must prioritize quality, set clear objectives, and integrate these with business goals. Effective management review processes are crucial.
Business Continuity: Establishments should develop robust plans to handle disruptions, ensuring consistent operations and supply chain reliability.
Advanced Pharmaceutical Quality System (PQS): Implementing quality principles like Quality by Design (QbD) and risk management approaches to maintain system reliability and minimize production disruptions.
Technical Excellence: Emphasizing data management, innovative manufacturing processes, and advanced technologies to enhance quality and operational efficiency.
Employee Engagement and Empowerment: Encouraging employees to take ownership of quality, make suggestions, and understand their impact on product quality and patient safety.
Implementation and Assessment
The FDA has developed a prototype assessment protocol to evaluate QMM. This includes a standardized approach to minimize bias and ensure objectivity. Someday, eventually, it will move away from constant prototyping.
Assessments will focus on qualitative aspects, such as the establishment’s quality culture and how it uses data to drive improvements.
Benefits of QMM
Enhanced Supply Chain Reliability: By adopting mature quality management practices, establishments can reduce the occurrence of quality-related failures. The fact shortages continue to be so damning to our industry is a huge wake-up call.
Proactive Continual Improvement: Encourages a proactive approach to quality management, leveraging technological advancements and integrated business operations.
Long-term Cost Savings: Investing in a mature quality culture can lead to fewer compliance issues, reduced inspection needs, and overall cost reductions.
Conclusion
The FDA’s QMM program aims to transform how pharmaceutical quality is perceived, measured, and rewarded. The program seeks to ensure a more reliable drug supply and better patient outcomes by fostering a strong quality culture and recognizing advanced practices. It should be seen as part of a 20-year commitment from the agency in alignment with its international partners.
There is no term more misused and misunderstood than “Phase Appropriate.” It is one of those terms that just about everyone involved in FDA-regulated industries has an opinion on and one where we all get tripped up.
What do we mean by phase?
Drug development can be divided into discovery, preclinical studies, clinical development, and market approval.
Each one of these phases is further broken down.
It is also important to remember that certain activities may start in earlier phases. For example, for manufacturing, tech transfer, and commercial manufacturing can start in Phase 3 (and more and more these days even 2!).
An investigational drug for use in a phase 1 study, as described in § 312.21(a) of this chapter, is subject to the statutory requirements set forth in 21 U.S.C. 351(a)(2)(B). The production of such drug is exempt from compliance with the regulations in part 211 of this chapter. However, this exemption does not apply to an investigational drug for use in a phase 1 study once the investigational drug has been made available for use by or for the sponsor in a phase 2 or phase 3 study, as described in § 312.21(b) and (c) of this chapter, or the drug has been lawfully marketed. If the investigational drug has been made available in a phase 2 or phase 3 study or the drug has been lawfully marketed, the drug for use in the phase 1 study must comply with part 211.
Guideline on the responsibilities of the sponsor with regard to handling and shipping of investigational medicinal products for human use in accordance with Good Clinical Practice and Good Manufacturing Practice
Processes characterized and Production and Process Controls (PPC) identified
Analytical methods are qualified
Materials acceptance criteria
Critical vendors qualified
Phase 3:
Processes validated with Production and Process Controls (PPC) identified and controlled
Validation of analytical methods
Materials have been fully qualified and tested upon receipt as appropriate
What About the Quality System?
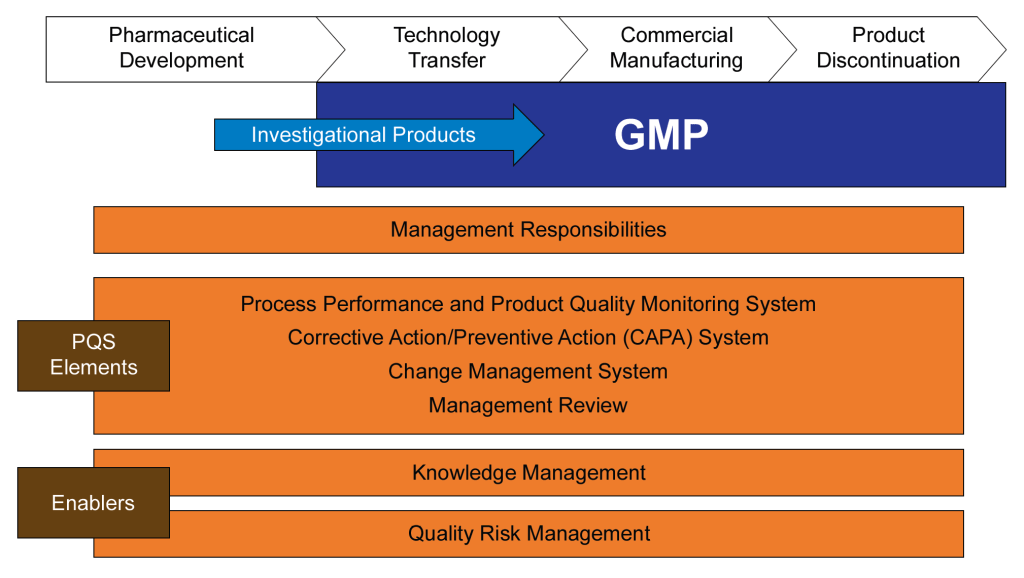
ICH Q10 clearly spells out the PQS requirements, breaking down into stages of Pharmaceutical Development (usually Phase 1 and earlier), Technology Transfer (usually phase 2), Commercial Manufacturing (which may start before approval) and Product Discontinuation. Q10 then lays out the expectations by these stages for the four key elements of:
Process performance and product quality monitoring system
Corrective action and preventive action (CAPA) system
Change management system
Management review of process performance and product quality.
Pharmaceutical Development
Technology Transfer
Commercial Manufacturing
Product Discontinuation
Process Performance and Product Quality
Process and product knowledge generated and process and product monitoring conducted throughout development can be used to establish a control strategy for manufacturing.
Monitoring during scale-up activities can provide a preliminary indication of process performance and the successful integration into manufacturing. Knowledge obtained during transfer and scale up activities can be useful in further developing the control strategy.
A well-defined system for process performance and product quality monitoring should be applied to assure performance within a state of control and to identify improvement areas.
Once manufacturing ceases, monitoring such as stability testing should continue to completion of the studies. Appropriate action on marketed product should continue to be executed according to regional regulations.
Corrective Action and Preventive Action
Product or process variability is explored. CAPA methodology is useful where corrective actions and preventive actions are incorporated into the iterative design and development process.
CAPA can be used as an effective system for feedback, feedforward and continual improvement.
CAPA should be used and the effectiveness of the actions should be evaluated.
CAPA should continue after the product is discontinued. The impact on product remaining on the market should be considered as well as other products which might be impacted.
Change Management
Change is an inherent part of the development process and should be documented; the formality of the change management process should be consistent with the stage of pharmaceutical development.
The change management system should provide management and documentation of adjustments made to the process during technology transfer activities.
A formal change management system should be in place for commercial manufacturing. Oversight by the quality unit should provide assurance of appropriate science and risk based assessments.
Any changes after product discontinuation should go through an appropriate change management system.
Management Review of Process Performance and Product Quality
Aspects of management review can be performed to ensure adequacy of the product and process design.
Aspects of management review should be performed to ensure the developed product and process can be manufactured at commercial scale.
Management review should be a structured system, as described above, and should support continual improvement.
Management review should include such items as product stability and product quality complaints.
ICH Stage appropriate quality system elements
Together with ICH Q9, this sets forth a framework of building knowledge and risk management into all aspects of the system together with a robust issue management mindset. There are really three things driving this.
Consistency in execution
Document decision making
Follow through
Some aspects remain pretty steady in all phases/stages, while others will grow as the organization develops.
The Difference Between Maturity and Phase Appropriate
People confuse phase appropriate with maturity all the time. Phase appropriate means doing the right activities in the right order. Maturity means the how is the most effective possible.
Quality Management Maturity (QMM) is the state attained when drug manufacturers have consistent, reliable, and robust business processes to achieve quality objectives and promote continual improvement. This is both composed of phase independent and phase dependent aspects.
Remember, a Quality Culture is the foundation that makes the rest of this happen.
A month back on LinkedIn I complained about a professional society pushing the idea of a document-free quality management system. This has got to be one of my favorite pet peeves that come from Industry 4.0 proponents, and it demonstrates a fundamental failure to understand core concepts. And frankly one of the reasons why many Industry/Quality/Pharma 4.0 initiatives truly fail to deliver. Unfortunately, I didn’t follow through with my idea of proposing a session to that conference, so instead here are my thoughts.
Fundamentally, documents are the lifeblood of an organization. But paper is not. This is where folks get confused. But fundamentally, this confusion is also limiting us.
Let’s go back to basics, which I covered in my 2018 post on document management.
When talking about documents, we really should talk about function and not just by name or type. This allows us to think more broadly about our documents and how they function as the lifeblood.
There are three types of documents:
Functional Documents provide instructions so people can perform tasks and make decisions safely effectively, compliantly, and consistently. This usually includes things like procedures, process instructions, protocols, methods, and specifications. Many of these need some sort of training decision. Functional documents should involve a process to ensure they are up-to-date, especially in relation to current practices and relevant standards (periodic review)
Records provide evidence that actions were taken, and decisions were made in keeping with procedures. This includes batch manufacturing records, logbooks and laboratory data sheets and notebooks. Records are a popular target for electronic alternatives.
Reports provide specific information on a particular topic on a formal, standardized way. Reports may include data summaries, findings, and actions to be taken.
The beating heart of our quality system brings us from functional to record to reports in a cycle of continuous improvement.
Functional documents are how we realize requirements, that is the needs and expectations of our organization. There are multiple ways to serve up the functional documents, the big three being paper, paper-on-glass, and some sort of execution system. That last, an execution system, united function with record, which is a big chunk of the promise of an execution system.
The maturation mind is to go from mostly paper execution, to paper-on-glass, to end-to-end integration and execution to drive up reliability and drive out error. But at the heart, we still have functional documents, records, and reports. Paper goes, but the document is there.
So how is this failing us?
Any process is a way to realize a set of requirements. Those requirements come from external (regulations, standards, etc) and internal (efficiency, business needs) sources. We then meet those requirements through People, Procedure, Principles, and Technology. They are interlinked and strive to deliver efficiency, effectiveness, and excellence.
So this failure to understand documents means we think we can solve this through a single technology application. an eQMS will solve problems in quality events, a LIMS for the lab, an MES for manufacturing. Each of these is a lever for change but alone cannot drive the results we want.
Because of the limitations of this thought process we get systems designed for yesterday’s problems, instead of thinking through towards tomorrow.
We get documentation systems that think of functional documents pretty much the same way we thought of them 30 years ago, as discrete things. These discrete things then interact through a gap with our electronic systems. There is little traceability, which complicates change control and makes it difficult to train experts. The funny thing, is we have the pieces, but because of the limitations of our technology we aren’t leveraging them.
The v-model approach should be leveraged in a risk-based manner to the design of our full system, and not just our technical aspects.
System feasibility matches policy and governance, user requirements allow us to trace to what elements are people, procedure, principles, and/or technology. Everything then stems from there.
Throughout the regulations and guidances you will find something like this: “As with other aspects of the development program, documentation may be ‘less vigorous’ in early phases, but ‘they would still need to be adequate in order to allow for traceability of the manufacturing process.'”
Agencies, like the FDA, have consistently stated that phase 1 is less vigorous but starting in phase 2 you are fully GMP. These regulations are meant to ensure basic safety and documentation standards are met in the manufacture and testing of phase 1 clinical trial material and to encourage the design of quality into the process. It is expected that enhanced process controls and GMP standards will be employed as the material transitions into later clinical stages.
With the speed of development, and the fact early phase material can support commercialization, this phased in approach is an important balancing act in advanced therapeutics like cell and gene therapy. It is crucial that manufacturers of phase 1 clinical trial material assess potential risks associated with their manufacturing process, facilities, equipment, methods, materials, etc. and the associated impact of these risks on the safety and quality of the material. All significant risks should then be mitigated, and appropriate controls implemented to reduce potential adverse impact for the patients and data generated.
Recognizing the difference between the elements of a strong quality system and what is needed for GMPs. Folks often confuse the two and have difficulties maturing quickly. The stuff in the orange? That’s system and is not GMP dependent.
Some GMP, such as clean room controls or starting materials controls should be robust from the beginning. Others, such as cleaning validation, are developed as you move through the phases.