The Catalent Indiana 483 form from July 2025 reads like a textbook example of my newest word, zemblanity, in risk management—the patterned, preventable misfortune that accrues not from blind chance, but from human agency and organizational design choices that quietly hardwire failure into our operations.
Twenty hair contamination deviations. Seven months to notify suppliers. Critical equipment failures dismissed as “not impacting SISPQ.” Media fill programs missing the very interventions they should validate. This isn’t random bad luck—it’s a quality system that has systematically normalized exactly the kinds of deviations that create inspection findings.
The Architecture of Inevitable Failure
Reading through the six major observations, three systemic patterns emerge that align perfectly with the hidden architecture of failure I discussed in my recent post on zemblanity.
Pattern 1: Investigation Theatre Over Causal Understanding
Observation 1 reveals what happens when investigations become compliance exercises rather than learning tools. The hair contamination trend—20 deviations spanning multiple product codes—received investigation resources proportional to internal requirement, not actual risk. As I’ve written about causal reasoning versus negative reasoning, these investigations focused on what didn’t happen rather than understanding the causal mechanisms that allowed hair to systematically enter sterile products.
The tribal knowledge around plunger seating issues exemplifies this perfectly. Operators developed informal workarounds because the formal system failed them, yet when this surfaced during an investigation, it wasn’t captured as a separate deviation worthy of systematic analysis. The investigation closed the immediate problem without addressing the systemic failure that created the conditions for operator innovation in the first place.
Pattern 2: Trend Blindness and Pattern Fragmentation
The most striking aspect of this 483 is how pattern recognition failed across multiple observations. Twenty-three work orders on critical air handling systems. Ten work orders on a single critical water system. Recurring membrane failures. Each treated as isolated maintenance issues rather than signals of systematic degradation.
This mirrors what I’ve discussed about normalization of deviance—where repeated occurrences of problems that don’t immediately cause catastrophe gradually shift our risk threshold. The work orders document a clear pattern of equipment degradation, yet each was risk-assessed as “not impacting SISPQ” without apparent consideration of cumulative or interactive effects.
Pattern 3: Control System Fragmentation
Perhaps most revealing is how different control systems operated in silos. Visual inspection systems that couldn’t detect the very defects found during manual inspection. Environmental monitoring that didn’t include the most critical surfaces. Media fills that omitted interventions documented as root causes of previous failures.
This isn’t about individual system inadequacy—it’s about what happens when quality systems evolve as collections of independent controls rather than integrated barriers designed to work together.
Solutions: From Zemblanity to Serendipity
Drawing from the approaches I’ve developed on this blog, here’s how Catalent could transform their quality system from one that breeds inevitable failure to one that creates conditions for quality serendipity:
Implement Causally Reasoned Investigations
The Energy Safety Canada white paper I discussed earlier this year offers a powerful framework for moving beyond counterfactual analysis. Instead of concluding that operators “failed to follow procedure” regarding stopper installation, investigate why the procedure was inadequate for the equipment configuration. Instead of noting that supplier notification was delayed seven months, understand the systemic factors that made immediate notification unlikely.
Practical Implementation:
Retrain investigators in causal reasoning techniques
Require investigation sponsors (area managers) to set clear expectations for causal analysis
Implement structured causal analysis tools like Cause-Consequence Analysis
Focus on what actually happened and why it made sense to people at the time
The take-the-best heuristic I recently explored offers a powerful lens for barrier analysis. Rather than implementing multiple independent controls, identify the single most causally powerful barrier that would prevent each failure type, then design supporting barriers that enhance rather than compete with the primary control.
For hair contamination specifically:
Implement direct stopper surface monitoring as the primary barrier
Design visual inspection systems specifically to detect proteinaceous particles
Create supplier qualification that includes contamination risk assessment
Establish real-time trend analysis linking supplier lots to contamination events
Establish Dynamic Trend Integration
Traditional trending treats each system in isolation—environmental monitoring trends, deviation trends, CAPA trends, maintenance trends. The Catalent 483 shows what happens when these parallel trend systems fail to converge into integrated risk assessment.
Integrated Trending Framework:
Create cross-functional trend review combining all quality data streams
Implement predictive analytics linking maintenance patterns to quality risks
Design Product Quality Reviews that explicitly correlate equipment performance with product quality data
Transform CAPA from Compliance to Learning
The recurring failures documented in this 483—repeated hair findings after CAPA implementation, continued equipment failures after “repair”—reflect what I’ve called the effectiveness paradox. Traditional CAPA focuses on thoroughness over causal accuracy.
CAPA Transformation Strategy:
Implement a proper CAPA hierarchy, prioritizing elimination and replacement over detection and mitigation
Establish effectiveness criteria before implementation, not after
Create learning-oriented CAPA reviews that ask “What did this teach us about our system?”
Link CAPA effectiveness directly to recurrence prevention rather than procedural compliance
Build Anticipatory Quality Architecture
The most sophisticated element would be creating what I call “quality serendipity”—systems that create conditions for positive surprises rather than inevitable failures. This requires moving from reactive compliance to anticipatory risk architecture.
Anticipatory Elements:
Implement supplier performance modeling that predicts contamination risk before it manifests
Create equipment degradation models that trigger quality assessment before failure
Establish operator feedback systems that capture emerging risks in real-time
Design quality reviews that explicitly seek weak signals of system stress
The Cultural Foundation
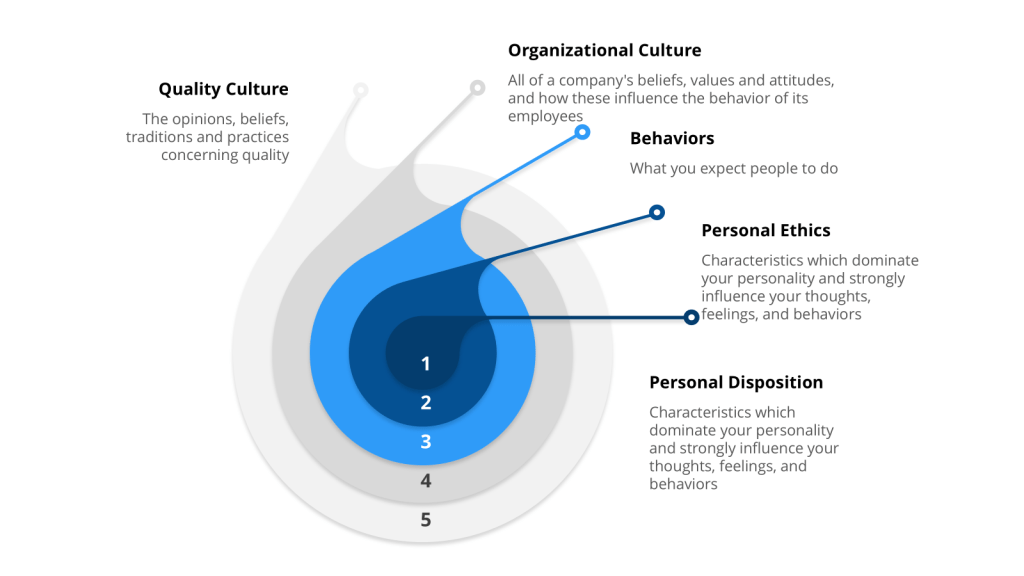
None of these technical solutions will work without addressing the cultural foundation that allowed this level of systematic failure to persist. The 483’s most telling detail isn’t any single observation—it’s the cumulative picture of an organization where quality indicators were consistently rationalized rather than interrogated.
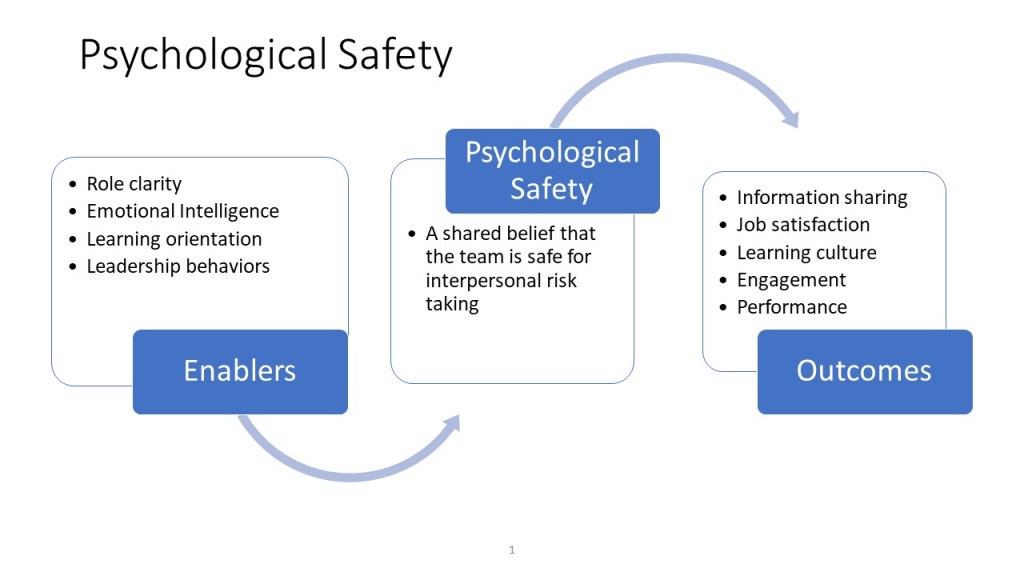
As I’ve written about quality culture, without psychological safety and learning orientation, people won’t commit to building and supporting robust quality systems. The tribal knowledge around plunger seating, the normalization of recurring equipment failures, the seven-month delay in supplier notification—these suggest a culture where adaptation to system inadequacy became preferable to system improvement.
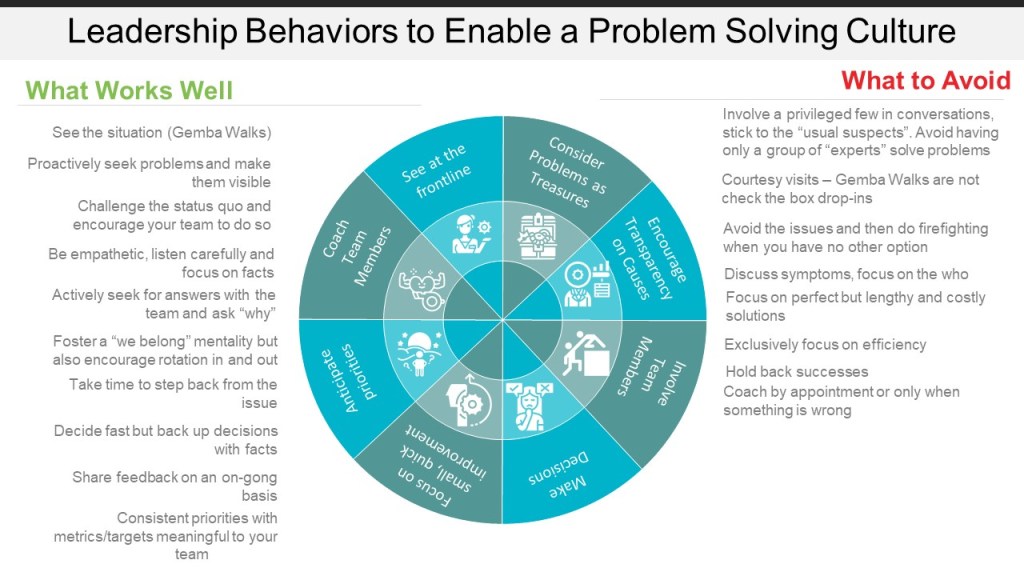
The path forward requires leadership that creates conditions for quality serendipity: reward pattern recognition over problem solving, celebrate early identification of weak signals, and create systems that make the right choice the easy choice.
Beyond Compliance: Building Anti-Fragile Quality
The Catalent 483 offers more than a cautionary tale—it provides a roadmap for quality transformation. Every observation represents an invitation to build quality systems that become stronger under stress rather than more brittle.
Organizations that master this transformation—moving from zemblanity-generating systems to serendipity-creating ones—will find that quality becomes not just a regulatory requirement but a competitive advantage. They’ll detect risks earlier, respond more effectively, and create the kind of operational resilience that turns disruption into opportunity.
The choice is clear: continue managing quality as a collection of independent compliance activities, or build integrated systems designed to create the conditions for sustained quality success. The Catalent case shows us what happens when we choose poorly. The frameworks exist to choose better.
What patterns of “inevitable failure” do you see in your own quality systems? How might shifting from negative reasoning to causal understanding transform your approach to investigations? Share your thoughts—this conversation about quality transformation is one we need to have across the industry.
The concept of “buying down risk” through operational capability development fundamentally depends on addressing the cognitive foundations that underpin effective risk assessment and decision-making. There are three critical systematic vulnerabilities that plague risk management processes: unjustified assumptions, incomplete identification of risks, and inappropriate use of risk assessment tools. These failures represent more than procedural deficiencies—they expose cognitive and knowledge management vulnerabilities that can undermine even the most well-intentioned quality systems.
Unjustified assumptions emerge when organizations rely on historical performance data or familiar process knowledge without adequately considering how changes in conditions, equipment, or supply chains might alter risk profiles. This manifests through anchoring bias, where teams place undue weight on initial information, leading to conclusions like “This process has worked safely for five years, so the risk profile remains unchanged.” Confirmation bias compounds this issue by causing assessors to seek information confirming existing beliefs while ignoring contradictory evidence.
Incomplete risk identification occurs when cognitive limitations and organizational biases inhibit comprehensive hazard recognition. Availability bias leads to overemphasis on dramatic but unlikely events while underestimating more probable but less memorable risks. Additionally, groupthink in risk assessment teams causes initial dissenting voices to be suppressed as consensus builds around preferred conclusions, limiting the scope of risks considered.
Inappropriate use of risk assessment tools represents the third systematic vulnerability, where organizations select methodologies based on familiarity rather than appropriateness for specific decision-making contexts. This includes using overly formal tools for trivial issues, applying generic assessment approaches without considering specific operational contexts, and relying on subjective risk scoring that provides false precision without meaningful insight. The misapplication often leads to risk assessments that fail to add value or clarity because they only superficially address root causes while generating high levels of subjectivity and uncertainty in outputs.
Traditional risk management approaches often focus on methodological sophistication while overlooking the cognitive realities that determine assessment effectiveness. Risk management operates fundamentally as a framework rather than a rigid methodology, providing structural architecture that enables systematic approaches to identifying, assessing, and controlling uncertainties. This framework distinction proves crucial because it recognizes that excellence emerges from the intersection of systematic process design with cognitive support systems that work with, rather than against, human decision-making patterns.
The Minimal Viable Risk Assessment Team: Beyond Compliance Theater
The foundation of cognitive excellence in risk management begins with assembling teams designed for cognitive rigor, knowledge depth, and psychological safety rather than mere compliance box-checking. The minimal viable risk assessment team concept challenges traditional approaches by focusing on four non-negotiable core roles that provide essential cognitive perspectives and knowledge anchors.
The Four Cognitive Anchors
Process Owner: The Reality Anchor represents lived operational experience rather than signature authority. This individual has engaged with the operation within the last 90 days and carries authority to change methods, budgets, and training. Authentic process ownership dismantles assumptions by grounding every risk statement in current operational facts, countering the tendency toward unjustified assumptions that plague many risk assessments.
Molecule Steward: The Patient’s Advocate moves beyond generic subject matter expertise to provide specific knowledge of how the particular product fails and can translate deviations into patient impact. When temperature drifts during freeze-drying, the molecule steward can explain whether a monoclonal antibody will aggregate or merely lose shelf life. Without this anchor, teams inevitably under-score hazards that never appear in generic assessment templates.
Technical System Owner: The Engineering Interpreter bridges the gap between equipment design intentions and operational realities. Equipment obeys physics rather than meeting minutes, and the system owner must articulate functional requirements, design limits, and engineering principles. This role prevents method-focused teams from missing systemic failures where engineering and design flaws could push entire batches outside critical parameters.
Quality Integrator: The Bias Disruptor forces cross-functional dialogue and preserves evidence of decision-making processes. Quality’s mission involves writing assumption logs, challenging confirmation bias, and ensuring dissenting voices are heard. This role maintains knowledge repositories so future teams are not condemned to repeat forgotten errors, directly addressing the knowledge management dimension of systematic risk assessment failure.
Knowledge Accessibility: The Missing Link in Risk Management
The Knowledge Accessibility Index (KAI) provides a systematic framework for evaluating how effectively organizations can access and deploy critical knowledge when decision-making requires specialized expertis. Unlike traditional knowledge management metrics focusing on knowledge creation or storage, the KAI specifically evaluates the availability, retrievability, and usability of knowledge at the point of decision-making.
Four Dimensions of Knowledge Accessibility
Expert Knowledge Availability assesses whether organizations can identify and access subject matter experts when specialized knowledge is required. This includes expert mapping and skill matrices, availability assessment during different operational scenarios, knowledge succession planning, and cross-training coverage for critical capabilities. The pharmaceutical environment demands that a qualified molecule steward be accessible within two hours for critical quality decisions, yet many organizations lack systematic approaches to ensuring this availability.
Knowledge Retrieval Efficiency measures how quickly and effectively teams can locate relevant information when making decisions. This encompasses search functionality effectiveness, knowledge organization and categorization, information architecture alignment with decision-making workflows, and access permissions balancing protection with accessibility. Time to find information represents a critical efficiency indicator that directly impacts the quality of risk assessment outcomes.
Knowledge Quality and Currency evaluates whether accessible knowledge is accurate, complete, and up-to-date through information accuracy verification processes, knowledge update frequency management, source credibility validation mechanisms, and completeness assessment relative to decision-making requirements. Outdated or incomplete knowledge can lead to systematic assessment failures even when expertise appears readily available.
Contextual Applicability assesses whether knowledge can be effectively applied to specific decision-making contexts through knowledge contextualization for operational scenarios, applicability assessment for different situations, integration capabilities with existing processes, and usability evaluation from end-user perspectives. Knowledge that exists but cannot be effectively applied provides little value during critical risk assessment activities.
Effective risk assessment team design fundamentally serves as knowledge preservation, not just compliance fulfillment. Every effective risk team is a living repository of organizational critical process insights, technical know-how, and operational experience. When teams include process owners, technical system engineers, molecule stewards, and quality integrators with deep hands-on familiarity, they collectively safeguard hard-won lessons and tacit knowledge that are often lost during organizational transitions.
Combating organizational forgetting requires intentional, cross-functional team design that fosters active knowledge transfer. When risk teams bring together diverse experts who routinely interact, challenge assumptions, and share context from respective domains, they create dynamic environments where critical information is surfaced, scrutinized, and retained. This living dialogue proves more effective than static records because it allows continuous updating and contextualization of knowledge in response to new challenges, regulatory changes, and operational shifts.
Team design becomes a strategic defense against the silent erosion of expertise that can leave organizations exposed to avoidable risks. By prioritizing teams that embody both breadth and depth of experience, organizations create robust safety nets that catch subtle warning signs, adapt to evolving risks, and ensure critical knowledge endures beyond individual tenure. This transforms collective memory into competitive advantage and foundation for sustained quality.
Cultural Integration: Embedding Cognitive Excellence
The development of truly effective risk management capabilities requires cultural transformation that embeds cognitive excellence principles into organizational DNA. Organizations with strong risk management cultures demonstrate superior capability in preventing quality issues, detecting problems early, and implementing effective corrective actions that address root causes rather than symptoms.
Psychological Safety as Cognitive Infrastructure
Psychological safety creates the foundational environment where personnel feel comfortable challenging assumptions, raising concerns about potential risks, and admitting uncertainty or knowledge limitations. This requires organizational cultures that treat questioning and systematic analysis as valuable contributions rather than obstacles to efficiency. Without psychological safety, the most sophisticated risk assessment methodologies and team compositions cannot overcome the fundamental barrier of information suppression.
Leaders must model vulnerability by sharing personal errors and how systems, not individuals, failed. They must invite dissent early in meetings with questions like “What might we be overlooking?” and reward candor by recognizing people who halt production over questionable trends. Psychological safety converts silent observers into active risk sensors, dramatically improving the effectiveness of knowledge accessibility and risk identification processes.
Structured Decision-Making as Cultural Practice
Excellence in pharmaceutical quality systems requires moving beyond hoping individuals will overcome cognitive limitations through awareness alone. Instead, organizations must design structured decision-making processes that systematically counter known biases while supporting comprehensive risk identification and analysis.
Forced systematic consideration involves checklists, templates, and protocols requiring teams to address specific risk categories and evidence types before reaching conclusions. Rather than relying on free-form discussion influenced by availability bias or groupthink, these tools ensure comprehensive coverage of relevant factors.
Devil’s advocate processes systematically introduce alternative perspectives and challenge preferred conclusions. By assigning specific individuals to argue against prevailing views or identify overlooked risks, organizations counter confirmation bias and overconfidence while identifying blind spots.
Staged decision-making separates risk identification from evaluation, preventing premature closure and ensuring adequate time for comprehensive hazard identification before moving to analysis and control decisions.
Implementation Framework: Building Cognitive Resilience
Phase 1: Knowledge Accessibility Audit
Organizations must begin with systematic knowledge accessibility audits that identify potential vulnerabilities in expertise availability and access. This audit addresses expertise mapping to identify knowledge holders and capabilities, knowledge accessibility assessment evaluating how effectively relevant knowledge can be accessed, knowledge quality evaluation assessing currency and completeness, and cognitive bias vulnerability assessment identifying situations where biases most likely affect conclusions.
For pharmaceutical manufacturing organizations, this audit might assess whether teams can access qualified molecule stewards within two hours for critical quality decisions, whether current system architecture documentation is accessible and comprehensible to risk assessment teams, whether process owners with recent operational experience are available for participation, and whether quality professionals can effectively challenge assumptions and integrate diverse perspectives.
Phase 2: Team Charter and Competence Framework
Moving from compliance theater to protection requires assembling teams with clear charters focused on cognitive rigor rather than checklist completion. An excellent risk team exists to frame, analyze, and communicate uncertainty so businesses can make science-based, patient-centered decisions. Before naming people, organizations must document the decisions teams must enable, the degree of formality those decisions demand, and the resources management will guarantee.
Competence proving rather than role filling ensures each core seat demonstrates documented capabilities. The process owner must have lived the operation recently with authority to change methods and budgets. The molecule steward must understand how specific products fail and translate deviations into patient impact. The technical system owner must articulate functional requirements and design limits. The quality integrator must force cross-functional dialogue and preserve evidence.
Phase 3: Knowledge System Integration
Knowledge-enabled decision making requires structures that make relevant information accessible at decision points while supporting cognitive processes necessary for accurate analysis. This involves structured knowledge capture that explicitly identifies assumptions, limitations, and context rather than simply documenting conclusions. Knowledge validation systems systematically test assumptions embedded in organizational knowledge, including processes for challenging accepted wisdom and updating mental models when new evidence emerges.
Expertise networks connect decision-makers with relevant specialized knowledge when required rather than relying on generalist teams for all assessments. Decision support systems prompt systematic consideration of potential biases and alternative explanations, creating technological infrastructure that supports rather than replaces human cognitive capabilities.
The final phase focuses on embedding cognitive excellence principles into organizational culture through systematic training programs that build both technical competencies and cognitive skills. These programs address not just what tools to use but how to think systematically about complex risk assessment challenges.
Continuous improvement mechanisms systematically analyze risk assessment performance to identify enhancement opportunities and implement improvements in methodologies, training, and support systems. Organizations track prediction accuracy, compare expected versus actual detectability, and feed insights into updated templates and training so subsequent teams start with enhanced capabilities.
Advanced Maturity: Predictive Risk Intelligence
Organizations achieving the highest levels of cognitive excellence implement predictive analytics, real-time bias detection, and adaptive systems that learn from assessment performance. These capabilities enable anticipation of potential risks and bias patterns before they manifest in assessment failures, including systematic monitoring of assessment performance, early warning systems for cognitive failures, and proactive adjustment of assessment approaches based on accumulated experience.
Adaptive learning systems continuously improve organizational capabilities based on performance feedback and changing conditions. These systems identify emerging patterns in risk assessment challenges and automatically adjust methodologies, training programs, and support systems to maintain effectiveness. Organizations at this maturity level contribute to industry knowledge and best practices while serving as benchmarks for other organizations.
From Reactive Compliance to Proactive Capability
The integration of cognitive science insights, knowledge accessibility frameworks, and team design principles creates a transformative approach to pharmaceutical risk management that moves beyond traditional compliance-focused activities toward strategic capability development. Organizations implementing these integrated approaches develop competitive advantages that extend far beyond regulatory compliance.
They build capabilities in systematic decision-making that improve performance across all aspects of pharmaceutical quality management. They create resilient systems that adapt to changing conditions while maintaining consistent effectiveness. Most importantly, they develop cultures of excellence that attract and retain exceptional talent while continuously improving capabilities.
The strategic integration of risk management practices with cultural transformation represents not merely an operational improvement opportunity but a fundamental requirement for sustained success in the evolving pharmaceutical manufacturing environment. Organizations implementing comprehensive risk buy-down strategies through systematic capability development will emerge as industry leaders capable of navigating regulatory complexity while delivering consistent value to patients, stakeholders, and society.
Excellence in this context means designing quality systems that work with human cognitive capabilities rather than against them. This requires integrating knowledge management principles with cognitive science insights to create environments where systematic, evidence-based decision-making becomes natural and sustainable. True elegance in quality system design comes from seamlessly integrating technical excellence with cognitive support, creating systems where the right decisions emerge naturally from the intersection of human expertise and systematic process.
Building Operational Capabilities Through Strategic Risk Management and Cultural Transformation
The Strategic Imperative: Beyond Compliance Theater
The fundamental shift from checklist-driven compliance to sustainable operational excellence grounded in robust risk management culture. Organizations continue to struggle with fundamental capability gaps that manifest as systemic compliance failures, operational disruptions, and ultimately, compromised patient safety.
The Risk Buy-Down Paradigm in Operations
The core challenge here is to build operational capabilities through proactively building systemic competencies that reduce the probability and impact of operational failures over time. Unlike traditional risk mitigation strategies that focus on reactive controls, risk buy-down emphasizes capability development that creates inherent resilience within operational systems.
This paradigm shifts the traditional cost-benefit equation from reactive compliance expenditure to proactive capability investment. Organizations implementing risk buy-down strategies recognize that upfront investments in operational excellence infrastructure generate compounding returns through reduced deviation rates, fewer regulatory observations, improved operational efficiency, and enhanced competitive positioning.
Economic Logic: Investment versus Failure Costs
The financial case for operational capability investment becomes stark when examining failure costs across the pharmaceutical industry. Drug development failures, inclusive of regulatory compliance issues, represent costs ranging from $500 to $900 million per program when accounting for capital costs and failure probabilities. Manufacturing quality failures trigger cascading costs including batch losses, investigation expenses, remediation efforts, regulatory responses, and market disruption.
Pharmaceutical manufacturers continue experiencing fundamental quality system failures despite decades of regulatory enforcement. These failures indicate insufficient investment in underlying operational capabilities, resulting in recurring compliance issues that generate exponentially higher long-term costs than proactive capability development would require.
Organizations successfully implementing risk buy-down strategies demonstrate measurable operational improvements. Companies with strong risk management cultures experience 30% higher likelihood of outperforming competitors while achieving 21% increases in productivity. These performance differentials reflect the compound benefits of systematic capability investment over reactive compliance expenditure.
Just look at the recent whitepaper published by the FDA to see the identified returns to this investment.
Regulatory Intelligence Framework Integration
The regulatory intelligence framework provides crucial foundation for risk buy-down implementation by enabling organizations to anticipate, assess, and proactively address emerging compliance requirements. Rather than responding reactively to regulatory observations, organizations with mature regulatory intelligence capabilities identify systemic capability gaps before they manifest as compliance violations.
Effective regulatory intelligence programs monitor FDA warning letter trends, 483 observations, and enforcement actions to identify patterns indicating capability deficiencies across industry segments. For example, persistent Quality Unit oversight failures across multiple geographic regions indicate fundamental organizational design issues rather than isolated procedural lapses8. This intelligence enables organizations to invest in Quality Unit empowerment, authority structures, and oversight capabilities before experiencing regulatory action.
The integration of regulatory intelligence with risk buy-down strategies creates a proactive capability development cycle where external regulatory trends inform internal capability investments, reducing both regulatory exposure and operational risk while enhancing competitive positioning through superior operational performance.
Culture as the Primary Risk Control
Organizational Culture as Foundational Risk Management
Organizational culture represents the most fundamental risk control mechanism within pharmaceutical operations, directly influencing how quality decisions are made, risks are identified and escalated, and operational excellence is sustained over time. Unlike procedural controls that can be circumvented or technical systems that can fail, culture operates as a pervasive influence that shapes behavior across all organizational levels and operational contexts.
Research demonstrates that organizations with strong risk management cultures are significantly less likely to experience damaging operational risk events and are better positioned to effectively respond when issues do occur.
The foundational nature of culture as a risk control becomes evident when examining quality system failures across pharmaceutical operations. Recent FDA warning letters consistently identify cultural deficiencies underlying technical violations, including insufficient Quality Unit authority, inadequate management commitment to compliance, and systemic failures in risk identification and escalation. These patterns indicate that technical compliance measures alone cannot substitute for robust quality culture.
Quality Culture Impact on Operational Resilience
Quality culture directly influences operational resilience by determining how organizations identify, assess, and respond to quality-related risks throughout manufacturing operations. Organizations with mature quality cultures demonstrate superior capability in preventing quality issues, detecting problems early, and implementing effective corrective actions that address root causes rather than symptoms.
Research in the biopharmaceutical industry reveals that integrating safety and quality cultures creates a unified “Resilience Culture” that significantly enhances organizational ability to sustain high-quality outcomes even under challenging conditions. This resilience culture is characterized by commitment to excellence, customer satisfaction focus, and long-term success orientation that transcends short-term operational pressures.
The operational impact of quality culture manifests through multiple mechanisms. Strong quality cultures promote proactive risk identification where employees at all levels actively surface potential quality concerns before they impact product quality. These cultures support effective escalation processes where quality issues receive appropriate priority regardless of operational pressures. Most importantly, mature quality cultures sustain continuous improvement mindsets where operational challenges become opportunities for systematic capability enhancement.
Dual-Approach Model: Leadership and Employee Ownership
Effective quality culture development requires coordinated implementation of top-down leadership commitment and bottom-up employee ownership, creating organizational alignment around quality principles and operational excellence. This dual-approach model recognizes that sustainable culture transformation cannot be achieved through leadership mandate alone, nor through grassroots initiatives without executive support.
Top-down leadership commitment establishes organizational vision, resource allocation, and accountability structures necessary for quality culture development. Research indicates that leadership commitment is vital for quality culture success and sustainability, with senior management responsible for initiating transformational change, setting quality vision, dedicating resources, communicating progress, and exhibiting visible support. Middle managers and supervisors ensure employees receive direct support and are held accountable to quality values.
Bottom-up employee ownership develops through empowerment, engagement, and competency development that enables staff to integrate quality considerations into daily operations. Organizations achieve employee ownership by incorporating quality into staff orientations, including quality expectations in job descriptions and performance appraisals, providing ongoing training opportunities, granting decision-making authority, and eliminating fear of consequences for quality-related concerns.
The integration of these approaches creates organizational conditions where quality culture becomes self-reinforcing. Leadership demonstrates commitment through resource allocation and decision-making priorities, while employees experience empowerment to make quality-focused decisions without fear of negative consequences for raising concerns or stopping production when quality issues arise.
Culture’s Role in Risk Identification and Response
Mature quality cultures fundamentally alter organizational approaches to risk identification and response by creating psychological safety for surfacing concerns, establishing systematic processes for risk assessment, and maintaining focus on long-term quality outcomes over short-term operational pressures. These cultural characteristics enable organizations to identify and address quality risks before they impact product quality or regulatory compliance.
Risk identification effectiveness depends critically on organizational culture that encourages transparency, values diverse perspectives, and rewards proactive concern identification. Research demonstrates that effective risk cultures promote “speaking up” where employees feel confident raising concerns and leaders demonstrate transparency in decision-making. This cultural foundation enables early risk detection that prevents minor issues from escalating into major quality failures.
Risk response effectiveness reflects cultural values around accountability, continuous improvement, and systematic problem-solving. Organizations with strong risk cultures implement thorough root cause analysis, develop comprehensive corrective and preventive actions, and monitor implementation effectiveness over time. These cultural practices ensure that risk responses address underlying causes rather than symptoms, preventing issue recurrence and building organizational learning capabilities.
The measurement of cultural risk management effectiveness requires systematic assessment of cultural indicators including employee engagement, incident reporting rates, management response to concerns, and the quality of corrective action implementation. Organizations tracking these cultural metrics can identify areas requiring improvement and monitor progress in cultural maturity over time.
Continuous Improvement Culture and Adaptive Capacity
Continuous improvement culture represents a fundamental organizational capability that enables sustained operational excellence through systematic enhancement of processes, systems, and capabilities over time. This culture creates adaptive capacity by embedding improvement mindsets, methodologies, and practices that enable organizations to evolve operational capabilities in response to changing requirements and emerging challenges.
Research demonstrates that continuous improvement culture significantly enhances operational performance through multiple mechanisms. Organizations with strong continuous improvement cultures experience increased employee engagement, higher productivity levels, enhanced innovation, and superior customer satisfaction. These performance improvements reflect the compound benefits of systematic capability development over time.
The development of continuous improvement culture requires systematic investment in employee competencies, improvement methodologies, data collection and analysis capabilities, and organizational learning systems. Organizations achieving mature improvement cultures provide training in improvement methodologies, establish improvement project pipelines, implement measurement systems that track improvement progress, and create recognition systems that reward improvement contributions.
Adaptive capacity emerges from continuous improvement culture through organizational learning mechanisms that capture knowledge from improvement projects, codify successful practices, and disseminate learning across the organization. This learning capability enables organizations to build institutional knowledge that improves response effectiveness to future challenges while preventing recurrence of past issues.
Integration with Regulatory Intelligence and Preventive Action
The integration of continuous improvement methodologies with regulatory intelligence capabilities creates proactive capability development systems that identify and address potential compliance issues before they manifest as regulatory observations. This integration represents advanced maturity in organizational quality management where external regulatory trends inform internal improvement priorities.
Regulatory intelligence provides continuous monitoring of FDA warning letters, 483 observations, enforcement actions, and guidance documents to identify emerging compliance trends and requirements. This intelligence enables organizations to anticipate regulatory expectations and proactively develop capabilities that address potential compliance gaps before they are identified through inspection.
Trending analysis of regulatory observations across industry segments reveals systemic capability gaps that multiple organizations experience. For example, persistent citations for Quality Unit oversight failures indicate industry-wide challenges in Quality Unit empowerment, authority structures, and oversight effectiveness. Organizations with mature regulatory intelligence capabilities use this trending data to assess their own Quality Unit capabilities and implement improvements before experiencing regulatory action.
The implementation of preventive action based on regulatory intelligence creates competitive advantage through superior regulatory preparedness while reducing compliance risk exposure. Organizations systematically analyzing regulatory trends and implementing capability improvements demonstrate regulatory readiness that supports inspection success and enables focus on operational excellence rather than compliance remediation.
The Integration Framework
Aligning Risk Management with Operational Capability Development
The strategic alignment of risk management principles with operational capability development creates synergistic organizational systems where risk identification enhances operational performance while operational excellence reduces risk exposure. This integration requires systematic design of management systems that embed risk considerations into operational processes while using operational data to inform risk management decisions.
Risk-based quality management approaches provide structured frameworks for integrating risk assessment with quality management processes throughout pharmaceutical operations. These approaches move beyond traditional compliance-focused quality management toward proactive systems that identify, assess, and mitigate quality risks before they impact product quality or regulatory compliance.
The implementation of risk-based approaches requires organizational capabilities in risk identification, assessment, prioritization, and mitigation that must be developed through systematic training, process development, and technology implementation. Organizations achieving mature risk-based quality management demonstrate superior performance in preventing quality issues, reducing deviation rates, and maintaining regulatory compliance.
Operational capability development supports risk management effectiveness by creating robust processes, competent personnel, and effective oversight systems that reduce the likelihood of risk occurrence while enhancing response effectiveness when risks do materialize. This capability development includes technical competencies, management systems, and organizational culture elements that collectively create operational resilience.
Efficiency-Excellence-Resilience Nexus
The strategic integration of efficiency, excellence, and resilience objectives creates organizational capabilities that simultaneously optimize resource utilization, maintain high-quality standards, and sustain performance under challenging conditions. This integration challenges traditional assumptions that efficiency and quality represent competing objectives, instead demonstrating that properly designed systems achieve superior performance across all dimensions.
Operational efficiency emerges from systematic elimination of waste, optimization of processes, and effective resource utilization that reduces operational costs while maintaining quality standards.
Operational excellence encompasses consistent achievement of high-quality outcomes through robust processes, competent personnel, and effective management systems.
Operational resilience represents the capability to maintain performance under stress, adapt to changing conditions, and recover effectively from disruptions. Resilience emerges from the integration of efficiency and excellence capabilities with adaptive capacity, redundancy planning, and organizational learning systems that enable sustained performance across varying conditions.
Measurement and Monitoring of Cultural Risk Management
The development of comprehensive measurement systems for cultural risk management enables organizations to track progress, identify improvement opportunities, and demonstrate the business value of culture investments. These measurement systems must capture both quantitative indicators of cultural effectiveness and qualitative assessments of cultural maturity across organizational levels.
Quantitative cultural risk management metrics include employee engagement scores, incident reporting rates, training completion rates, corrective action effectiveness measures, and regulatory compliance indicators. These metrics provide objective measures of cultural performance that can be tracked over time and benchmarked against industry standards.
Qualitative cultural assessment approaches include employee surveys, focus groups, management interviews, and observational assessments that capture cultural nuances not reflected in quantitative metrics. These qualitative approaches provide insights into cultural strengths, improvement opportunities, and the effectiveness of cultural transformation initiatives.
The integration of quantitative and qualitative measurement approaches creates comprehensive cultural assessment capabilities that inform management decision-making while demonstrating progress in cultural maturity. Organizations with mature cultural measurement systems can identify cultural risk indicators early, implement targeted interventions, and track improvement effectiveness over time.
Risk culture measurement frameworks must align with organizational risk appetite, regulatory requirements, and business objectives to ensure relevance and actionability. Effective frameworks establish clear definitions of desired cultural behaviors, implement systematic measurement processes, and create feedback mechanisms that inform continuous improvement in cultural effectiveness.
Common Capability Gaps Revealed Through FDA Observations
Analysis of FDA warning letters and 483 observations reveals persistent capability gaps across pharmaceutical manufacturing operations that reflect systemic weaknesses in organizational design, management systems, and quality culture. These capability gaps manifest as recurring regulatory observations that persist despite repeated enforcement actions, indicating fundamental deficiencies in operational capabilities rather than isolated procedural failures.
Quality Unit oversight failures represent the most frequently cited deficiency in FDA warning letters. These failures encompass insufficient authority to ensure CGMP compliance, inadequate resources for effective oversight, poor documentation practices, and systematic failures in deviation investigation and corrective action implementation. The persistence of Quality Unit deficiencies across multiple geographic regions indicates industry-wide challenges in Quality Unit design and empowerment.
Data integrity violations represent another systematic capability gap revealed through regulatory observations, including falsified records, inappropriate data manipulation, deleted electronic records, and inadequate controls over data generation and review. These violations indicate fundamental weaknesses in data governance systems, personnel training, and organizational culture around data integrity principles.
Deviation investigation and corrective action deficiencies appear consistently across FDA warning letters, reflecting inadequate capabilities in root cause analysis, corrective action development, and implementation effectiveness monitoring. These deficiencies indicate systematic weaknesses in problem-solving methodologies, investigation competencies, and management systems for tracking corrective action effectiveness.
Manufacturing process control deficiencies including inadequate validation, insufficient process monitoring, and poor change control implementation represent persistent capability gaps that directly impact product quality and regulatory compliance. These deficiencies reflect inadequate technical capabilities, insufficient management oversight, and poor integration between manufacturing and quality systems.
GMP Culture Translation to Operational Resilience
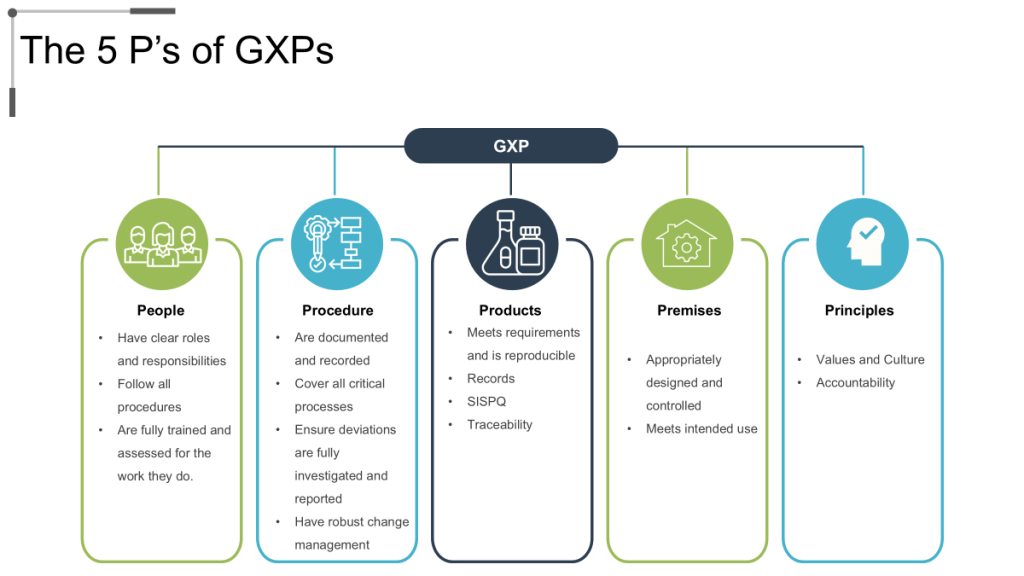
The five pillars of GMP – People, Product, Process, Procedures, and Premises – provide comprehensive framework for organizational capability development that addresses all aspects of pharmaceutical manufacturing operations. Effective GMP culture ensures that each pillar receives appropriate attention and investment while maintaining integration across all operational elements.
Personnel competency development represents the foundational element of GMP culture, encompassing technical training, quality awareness, regulatory knowledge, and continuous learning capabilities that enable employees to make appropriate quality decisions across varying operational conditions. Organizations with mature GMP cultures invest systematically in personnel development while creating career advancement opportunities that retain quality expertise.
Process robustness and validation ensure that manufacturing operations consistently produce products meeting quality specifications while providing confidence in process capability under normal operating conditions. GMP culture emphasizes process understanding, validation effectiveness, and continuous monitoring that enables proactive identification and resolution of process issues before they impact product quality.
Documentation systems and data integrity support all aspects of GMP implementation by providing objective evidence of compliance with regulatory requirements while enabling effective investigation and corrective action when issues occur. Mature GMP cultures emphasize documentation accuracy, completeness, and accessibility while implementing controls that prevent data integrity issues.
Risk-Based Quality Management as Operational Capability
Risk-based quality management represents advanced organizational capability that integrates risk assessment principles with quality management processes to create proactive systems that prevent quality issues while optimizing resource allocation. This capability enables organizations to focus quality oversight activities on areas with greatest potential impact while maintaining comprehensive quality assurance across all operations.
The implementation of risk-based quality management requires organizational capabilities in risk identification, assessment, prioritization, and mitigation that must be developed through systematic training, process development, and technology implementation. Organizations achieving mature risk-based capabilities demonstrate superior performance in preventing quality issues, reducing deviation rates, and maintaining regulatory compliance efficiency.
Critical process identification and control strategy development represent core competencies in risk-based quality management that enable organizations to focus resources on processes with greatest potential impact on product quality. These competencies require deep process understanding, risk assessment capabilities, and systematic approaches to control strategy optimization.
Continuous monitoring and trending analysis capabilities enable organizations to identify emerging quality risks before they impact product quality while providing data for systematic improvement of risk management effectiveness. These capabilities require data collection systems, analytical competencies, and management processes that translate monitoring results into proactive risk mitigation actions.
Supplier Management and Third-Party Risk Capabilities
Supplier management and third-party risk management represent critical organizational capabilities that directly impact product quality, regulatory compliance, and operational continuity. The complexity of pharmaceutical supply chains requires sophisticated approaches to supplier qualification, performance monitoring, and risk mitigation that go beyond traditional procurement practices.
Supplier qualification processes must assess not only technical capabilities but also quality culture, regulatory compliance history, and risk management effectiveness of potential suppliers. This assessment requires organizational capabilities in audit planning, execution, and reporting that provide confidence in supplier ability to meet pharmaceutical quality requirements consistently.
Performance monitoring systems must track supplier compliance with quality requirements, delivery performance, and responsiveness to quality issues over time. These systems require data collection capabilities, analytical competencies, and escalation processes that enable proactive management of supplier performance issues before they impact operations.
Risk mitigation strategies must address potential supply disruptions, quality failures, and regulatory compliance issues across the supplier network. Effective risk mitigation requires contingency planning, alternative supplier development, and inventory management strategies that maintain operational continuity while ensuring product quality.
The integration of supplier management with internal quality systems creates comprehensive quality assurance that extends across the entire value chain while maintaining accountability for product quality regardless of manufacturing location or supplier involvement. This integration requires organizational capabilities in supplier oversight, quality agreement management, and cross-functional coordination that ensure consistent quality standards throughout the supply network.
Implementation Roadmap for Cultural Risk Management Development
Staged Approach to Cultural Risk Management Development
The implementation of cultural risk management requires systematic, phased approach that builds organizational capabilities progressively while maintaining operational continuity and regulatory compliance. This staged approach recognizes that cultural transformation requires sustained effort over extended timeframes while providing measurable progress indicators that demonstrate value and maintain organizational commitment.
Phase 1: Foundation Building and Assessment establishes baseline understanding of current culture state, identifies immediate improvement opportunities, and creates infrastructure necessary for systematic cultural development. This phase includes comprehensive cultural assessment, leadership commitment establishment, initial training program development, and quick-win implementation that demonstrates early value from cultural investment.
Cultural assessment activities encompass employee surveys, management interviews, process observations, and regulatory compliance analysis that provide comprehensive understanding of current cultural strengths and improvement opportunities. These assessments establish baseline measurements that enable progress tracking while identifying specific areas requiring focused attention during subsequent phases.
Leadership commitment development ensures that senior management understands cultural transformation requirements, commits necessary resources, and demonstrates visible support for cultural change initiatives. This commitment includes resource allocation, communication of cultural expectations, and integration of cultural objectives into performance management systems.
Phase 2: Capability Development and System Implementation focuses on building specific competencies, implementing systematic processes, and creating organizational infrastructure that supports sustained cultural improvement. This phase includes comprehensive training program rollout, process improvement implementation, measurement system development, and initial culture champion network establishment.
Training program implementation provides employees with knowledge, skills, and tools necessary for effective participation in cultural transformation while creating shared understanding of quality expectations and risk management principles. These programs must be tailored to specific roles and responsibilities while maintaining consistency in core cultural messages.
Process improvement implementation creates systematic approaches to risk identification, assessment, and mitigation that embed cultural values into daily operations. These processes include structured problem-solving methodologies, escalation procedures, and continuous improvement practices that reinforce cultural expectations through routine operational activities.
Phase 3: Integration and Sustainment emphasizes cultural embedding, performance optimization, and continuous improvement capabilities that ensure long-term cultural effectiveness. This phase includes advanced measurement system implementation, culture champion network expansion, and systematic review processes that maintain cultural momentum over time.
Leadership Engagement Strategies for Sustainable Change
Leadership engagement represents the most critical factor in successful cultural transformation, requiring systematic strategies that ensure consistent leadership behavior, effective communication, and sustained commitment throughout the transformation process. Effective leadership engagement creates organizational conditions where cultural change becomes self-reinforcing while providing clear direction and resources necessary for transformation success.
Visible Leadership Commitment requires leaders to demonstrate cultural values through daily decisions, resource allocation priorities, and personal behavior that models expected cultural norms. This visibility includes regular communication of cultural expectations, participation in cultural activities, and recognition of employees who exemplify desired cultural behaviors.
Leadership communication strategies must provide clear, consistent messages about cultural expectations while demonstrating transparency in decision-making and responsiveness to employee concerns. Effective communication includes regular updates on cultural progress, honest discussion of challenges, and celebration of cultural achievements that reinforce the value of cultural investment.
Leadership Development Programs ensure that managers at all levels possess competencies necessary for effective cultural leadership including change management skills, coaching capabilities, and performance management approaches that support cultural transformation. These programs must be ongoing rather than one-time events to ensure sustained leadership effectiveness.
Change management competencies enable leaders to guide employees through cultural transformation while addressing resistance, maintaining morale, and sustaining momentum throughout extended change processes. These competencies include stakeholder engagement, communication planning, and resistance management approaches that facilitate smooth cultural transitions.
Accountability Systems ensure that leaders are held responsible for cultural outcomes within their areas of responsibility while providing support and resources necessary for cultural success. These systems include cultural metrics integration into performance management systems, regular cultural assessment processes, and recognition programs that reward effective cultural leadership.
Training and Development Frameworks
Comprehensive training and development frameworks provide employees with competencies necessary for effective participation in risk-based quality culture while creating organizational learning capabilities that support continuous cultural improvement. These frameworks must be systematic, role-specific, and continuously updated to reflect evolving regulatory requirements and organizational capabilities.
Foundational Training Programs establish basic understanding of quality principles, risk management concepts, and regulatory requirements that apply to all employees regardless of specific role or function. This training creates shared vocabulary and understanding that enables effective cross-functional collaboration while ensuring consistent application of cultural principles.
Quality fundamentals training covers basic concepts including customer focus, process thinking, data-driven decision making, and continuous improvement that form the foundation of quality culture. This training must be interactive, practical, and directly relevant to employee daily responsibilities to ensure engagement and retention.
Risk management training provides employees with capabilities in risk identification, assessment, communication, and escalation that enable proactive risk management throughout operations. This training includes both conceptual understanding and practical tools that employees can apply immediately in their work environment.
Role-Specific Advanced Training develops specialized competencies required for specific positions while maintaining alignment with overall cultural objectives and organizational quality strategy. This training addresses technical competencies, leadership skills, and specialized knowledge required for effective performance in specific roles.
Management training focuses on leadership competencies, change management skills, and performance management approaches that support cultural transformation while achieving operational objectives. This training must be ongoing and include both formal instruction and practical application opportunities.
Technical training ensures that employees possess current knowledge and skills required for effective job performance while maintaining awareness of evolving regulatory requirements and industry best practices. This training includes both initial competency development and ongoing skill maintenance programs.
Continuous Learning Systems create organizational capabilities for identifying training needs, developing training content, and measuring training effectiveness that ensure sustained competency development over time. These systems include needs assessment processes, content development capabilities, and effectiveness measurement approaches that continuously improve training quality.
Metrics and KPIs for Tracking Capability Maturation
Comprehensive measurement systems for cultural capability maturation provide objective evidence of progress while identifying areas requiring additional attention and investment. These measurement systems must balance quantitative indicators with qualitative assessments to capture the full scope of cultural development while providing actionable insights for continuous improvement.
Leading Indicators measure cultural inputs and activities that predict future cultural performance including training completion rates, employee engagement scores, participation in improvement activities, and leadership behavior assessments. These indicators provide early warning of cultural issues while demonstrating progress in cultural development activities.
Employee engagement measurements capture employee commitment to organizational objectives, satisfaction with work environment, and confidence in organizational leadership that directly influence cultural effectiveness. These measurements include regular survey processes, focus group discussions, and exit interview analysis that provide insights into employee perspectives on cultural development.
Training effectiveness indicators track not only completion rates but also competency development, knowledge retention, and application of training content in daily work activities. These indicators ensure that training investments translate into improved job performance and cultural behavior.
Lagging Indicators measure cultural outcomes including quality performance, regulatory compliance, operational efficiency, and customer satisfaction that reflect the ultimate impact of cultural investments. These indicators provide validation of cultural effectiveness while identifying areas where cultural development has not yet achieved desired outcomes.
Quality performance metrics include deviation rates, customer complaints, product recalls, and regulatory observations that directly reflect the effectiveness of quality culture in preventing quality issues. These metrics must be trended over time to identify improvement patterns and areas requiring additional attention.
Operational efficiency indicators encompass productivity measures, cost performance, delivery performance, and resource utilization that demonstrate the operational impact of cultural improvements. These indicators help demonstrate the business value of cultural investments while identifying opportunities for further improvement.
Integrated Measurement Systems combine leading and lagging indicators into comprehensive dashboards that provide management with complete visibility into cultural development progress while enabling data-driven decision making about cultural investments. These systems include automated data collection, trend analysis capabilities, and exception reporting that focus management attention on areas requiring intervention.
Benchmarking capabilities enable organizations to compare their cultural performance against industry standards and best practices while identifying opportunities for improvement. These capabilities require access to industry data, analytical competencies, and systematic comparison processes that inform cultural development strategies.
Future-Facing Implications for the Evolving Regulatory Landscape
Emerging Regulatory Trends and Capability Requirements
The regulatory landscape continues evolving toward increased emphasis on risk-based approaches, data integrity requirements, and organizational culture assessment that require corresponding evolution in organizational capabilities and management approaches. Organizations must anticipate these regulatory developments and proactively develop capabilities that address future requirements rather than merely responding to current regulations.
Enhanced Quality Culture Focus in regulatory inspections requires organizations to demonstrate not only technical compliance but also cultural effectiveness in sustaining quality performance over time. This trend requires development of cultural measurement capabilities, cultural audit processes, and systematic approaches to cultural development that provide evidence of cultural maturity to regulatory inspectors.
Risk-based inspection approaches focus regulatory attention on areas with greatest potential risk while requiring organizations to demonstrate effective risk management capabilities throughout their operations. This evolution requires mature risk assessment capabilities, comprehensive risk mitigation strategies, and systematic documentation of risk management effectiveness.
Technology Integration and Cultural Adaptation
Technology integration in pharmaceutical manufacturing creates new opportunities for operational excellence while requiring cultural adaptation that maintains human oversight and decision-making capabilities in increasingly automated environments. Organizations must develop cultural approaches that leverage technology capabilities while preserving the human judgment and oversight essential for quality decision-making.
Digital quality systems enable real-time monitoring, advanced analytics, and automated decision support that enhance quality management effectiveness while requiring new competencies in system operation, data interpretation, and technology-assisted decision making. Cultural adaptation must ensure that technology enhances rather than replaces human quality oversight capabilities.
Data Integrity in Digital Environments requires sophisticated understanding of electronic systems, data governance principles, and cybersecurity requirements that go beyond traditional paper-based quality systems. Cultural development must emphasize data integrity principles that apply across both electronic and paper systems while building competencies in digital data management.
Building Adaptive Organizational Capabilities
The increasing pace of change in regulatory requirements, technology capabilities, and market conditions requires organizational capabilities that enable rapid adaptation while maintaining operational stability and quality performance. These adaptive capabilities must be embedded in organizational culture and management systems to ensure sustained effectiveness across changing conditions.
Learning Organization Capabilities enable systematic capture, analysis, and dissemination of knowledge from operational experience, regulatory changes, and industry developments that inform continuous organizational improvement. These capabilities include knowledge management systems, learning processes, and cultural practices that promote organizational learning and adaptation.
Scenario planning and contingency management capabilities enable organizations to anticipate potential future conditions and develop response strategies that maintain operational effectiveness across varying circumstances. These capabilities require analytical competencies, strategic planning processes, and risk management approaches that address uncertainty systematically.
Change Management Excellence encompasses systematic approaches to organizational change that minimize disruption while maximizing adoption of new capabilities and practices. These capabilities include change planning, stakeholder engagement, communication strategies, and performance management approaches that facilitate smooth organizational transitions.
Resilience building requires organizational capabilities that enable sustained performance under stress, rapid recovery from disruptions, and systematic strengthening of organizational capabilities based on experience with challenges. These capabilities encompass redundancy planning, crisis management, business continuity, and systematic approaches to capability enhancement based on lessons learned.
The future pharmaceutical manufacturing environment will require organizations that combine operational excellence with adaptive capability, regulatory intelligence with proactive compliance, and technical competence with robust quality culture. Organizations successfully developing these integrated capabilities will achieve sustainable competitive advantage while contributing to improved patient outcomes through reliable access to high-quality pharmaceutical products.
The strategic integration of risk management practices with cultural transformation represents not merely an operational improvement opportunity but a fundamental requirement for sustained success in the evolving pharmaceutical manufacturing environment. Organizations implementing comprehensive risk buy-down strategies through systematic capability development will emerge as industry leaders capable of navigating regulatory complexity while delivering consistent value to patients, stakeholders, and society.
Energy Safety Canada recently published a white paper on causal reasoning that offers valuable insights for quality professionals across industries. As someone who has spent decades examining how we investigate deviations and perform root cause analysis, I found their framework refreshing and remarkably aligned with the challenges we face in pharmaceutical quality. The paper proposes a fundamental shift in how we approach investigations, moving from what they call “negative reasoning” to “causal reasoning” that could significantly improve our ability to prevent recurring issues and drive meaningful improvement.
The Problem with Traditional Root Cause Analysis
Many of us in quality have experienced the frustration of seeing the same types of deviations recur despite thorough investigations and seemingly robust CAPAs. The Energy Safety Canada white paper offers a compelling explanation for this phenomenon: our investigations often focus on what did not happen rather than what actually occurred.
This approach, which the authors term “negative reasoning,” leads investigators to identify counterfactuals-things that did not occur, such as “operators not following procedures” or “personnel not stopping work when they should have”. The problem is fundamental: what was not happening cannot create the outcomes we experienced. As the authors aptly state, these counterfactuals “exist only in retrospection and never actually influenced events,” yet they dominate many of our investigation conclusions.
This insight resonates strongly with what I’ve observed in pharmaceutical quality. Six years ago the MHRA’s 2019 citation of 210 companies for inadequate root cause analysis and CAPA development – including 6 critical findings – takes on renewed significance in light of Sanofi’s 2025 FDA warning letter. While most cited organizations likely believed their investigation processes were robust (as Sanofi presumably did before their contamination failures surfaced), these parallel cases across regulatory bodies and years expose a persistent industry-wide disconnect between perceived and actual investigation effectiveness. These continued failures exemplify how superficial root cause analysis creates dangerous illusions of control – precisely the systemic flaw the MHRA data highlighted six years prior.
Negative Reasoning vs. Causal Reasoning: A Critical Distinction
The white paper makes a distinction that I find particularly valuable: negative reasoning seeks to explain outcomes based on what was missing from the system, while causal reasoning looks for what was actually present or what happened. This difference may seem subtle, but it fundamentally changes the nature and outcomes of our investigations.
When we use negative reasoning, we create what the white paper calls “an illusion of cause without being causal”. We identify things like “failure to follow procedures” or “inadequate risk assessment,” which may feel satisfying but don’t explain why those conditions existed in the first place. These conclusions often lead to generic corrective actions that fail to address underlying issues.
In contrast, causal reasoning requires statements that have time, place, and magnitude. It focuses on what was necessary and sufficient to create the effect, building a logically tight cause-and-effect diagram. This approach helps reveal how work is actually done rather than comparing reality to an imagined ideal.
This distinction parallels the gap between “work-as-imagined” (the black line) and “work-as-done” (the blue line). Too often, our investigations focus only on deviations from work-as-imagined without trying to understand why work-as-done developed differently.
A Tale of Two Analyses: The Power of Causal Reasoning
The white paper presents a compelling case study involving a propane release and operator injury that illustrates the difference between these two approaches. When initially analyzed through negative reasoning, investigators concluded the operator:
Used an improper tool
Deviated from good practice
Failed to recognize hazards
Failed to learn from past experiences
These conclusions placed blame squarely on the individual and led leadership to consider terminating the operator.
However, when the same incident was examined through causal reasoning, a different picture emerged:
The operator used the pipe wrench because it was available at the pump specifically for this purpose
The pipe wrench had been deliberately left at that location because operators knew the valve was hard to close
The operator acted quickly because he perceived a risk to the plant and colleagues
Leadership had actually endorsed this workaround four years earlier during a turnaround
This causally reasoned analysis revealed that what appeared to be an individual failure was actually a system-level issue that had been normalized over time. Rather than punishing the operator, leadership recognized their own role in creating the conditions for the incident and implemented systemic improvements.
This example reminded me of our discussions on barrier analysis, where we examine barriers that failed, weren’t used, or didn’t exist. But causal reasoning takes this further by exploring why those conditions existed in the first place, creating a much richer understanding of how work actually happens.
First 24 Hours: Where Causal Reasoning Meets The Golden Day
In my recent post on “The Golden Start to a Deviation Investigation,” I emphasized how critical the first 24 hours are after discovering a deviation. This initial window represents our best opportunity to capture accurate information and set the stage for a successful investigation. The Energy Safety Canada white paper complements this concept perfectly by providing guidance on how to use those critical hours effectively.
When we apply causal reasoning during these early stages, we focus on collecting specific, factual information about what actually occurred rather than immediately jumping to what should have happened. This means documenting events with specificity (time, place, magnitude) and avoiding premature judgments about deviations from procedures or expectations.
As I’ve previously noted, clear and precise problem definition forms the foundation of any effective investigation. Causal reasoning enhances this process by ensuring we document using specific, factual language that describes what occurred rather than what didn’t happen. This creates a much stronger foundation for the entire investigation.
Beyond Human Error: System Thinking and Leadership’s Role
One of the most persistent challenges in our field is the tendency to attribute events to “human error.” As I’ve discussed before, when human error is suspected or identified as the cause, this should be justified only after ensuring that process, procedural, or system-based errors have not been overlooked. The white paper reinforces this point, noting that human actions and decisions are influenced by the system in which people work.
In fact, the paper presents a hierarchy of causes that resonates strongly with systems thinking principles I’ve advocated for previously. Outcomes arise from physical mechanisms influenced by human actions and decisions, which are in turn governed by systemic factors. If we only address physical mechanisms or human behaviors without changing the system, performance will eventually migrate back to where it has always been.
This connects directly to what I’ve written about quality culture being fundamental to providing quality. The white paper emphasizes that leadership involvement is directly correlated with performance improvement. When leaders engage to set conditions and provide resources, they create an environment where investigations can reveal systemic issues rather than just identify procedural deviations or human errors.
Implementing Causal Reasoning in Pharmaceutical Quality
For pharmaceutical quality professionals looking to implement causal reasoning in their investigation processes, I recommend starting with these practical steps:
1. Develop Investigator Competencies
As I’ve discussed in my analysis of Sanofi’s FDA warning letter, having competent investigators is crucial. Organizations should:
Define required competencies for investigators
Provide comprehensive training on causal reasoning techniques
Implement mentoring programs for new investigators
Regularly assess and refresh investigator skills
2. Shift from Counterfactuals to Causal Statements
Review your recent investigations and look for counterfactual statements like “operators did not follow the procedure.” Replace these with causal statements that describe what actually happened and why it made sense to the people involved at the time.
3. Implement a Sponsor-Driven Approach
The white paper emphasizes the importance of investigation sponsors (otherwise known as Area Managers) who set clear conditions and expectations. This aligns perfectly with my belief that quality culture requires alignment between top management behavior and quality system philosophy. Sponsors should:
Clearly define the purpose and intent of investigations
Specify that a causal reasoning orientation should be used
Provide resources and access needed to find data and translate it into causes
Remain engaged throughout the investigation process
4. Use Structured Causal Analysis Tools
While the M-based frameworks I’ve discussed previously (4M, 5M, 6M) remain valuable for organizing contributing factors, they should be complemented with tools that support causal reasoning. The Cause-Consequence Analysis (CCA) I described in a recent post offers one such approach, combining elements of fault tree analysis and event tree analysis to provide a holistic view of risk scenarios.
From Understanding to Improvement
The Energy Safety Canada white paper’s emphasis on causal reasoning represents a valuable contribution to how we think about investigations across industries. For pharmaceutical quality professionals, this approach offers a way to move beyond compliance-focused investigations to truly understand how our systems operate and how to improve them.
As the authors note, “The capacity for an investigation to improve performance is dependent on the type of reasoning used by investigators”. By adopting causal reasoning, we can build investigations that reveal how work actually happens rather than simply identifying deviations from how we imagine it should happen.
This approach aligns perfectly with my long-standing belief that without a strong quality culture, people will not be ready to commit and involve themselves fully in building and supporting a robust quality management system. Causal reasoning creates the transparency and learning that form the foundation of such a culture.
I encourage quality professionals to download and read the full white paper, reflect on their current investigation practices, and consider how causal reasoning might enhance their approach to understanding and preventing deviations. The most important questions to consider are:
Do your investigation conclusions focus on what didn’t happen rather than what did?
How often do you identify “human error” without exploring the system conditions that made that error likely?
Are your leaders engaged as sponsors who set conditions for successful investigations?
What barriers exist in your organization that prevent learning from events?
As we continue to evolve our understanding of quality and safety, approaches like causal reasoning offer valuable tools for creating the transparency needed to navigate complexity and drive meaningful improvement.
How you respond in the first 24 hours after discovering a deviation can make the difference between a minor quality issue and a major compliance problem. This critical window-what I call “The Golden Day”-represents your best opportunity to capture accurate information, contain potential risks, and set the stage for a successful investigation. When managed effectively, this initial day creates the foundation for identifying true root causes and implementing effective corrective actions that protect product quality and patient safety.
Why the First 24 Hours Matter: The Evidence
The initial response to a deviation is crucial for both regulatory compliance and effective problem-solving. Industry practice and regulatory expectations align on the importance of quick, systematic responses to deviations.
Regulatory expectations explicitly state that deviation investigation and root cause determination should be completed in a timely manner, and industry expectations usually align on deviations being completed within 30 days of discovery.
In the landmark U.S. v. Barr Laboratories case, “the Court declared that all failure investigations must be performed promptly, within thirty business days of the problem’s occurrence”
Best practices recommend assembling a cross-functional team immediately after deviation discovery and conduct initial risk assessment within 24 hours”
Initial actions taken in the first day directly impact the quality and effectiveness of the entire investigation process
When you capitalize on this golden window, you’re working with fresh memories, intact evidence, and the highest chance of observing actual conditions that contributed to the deviation.
Clear, precise problem definition forms the foundation of any effective investigation. Vague or incomplete problem statements lead to misdirected investigations and ultimately, inadequate corrective actions.
Document using specific, factual language that describes what occurred versus what was expected
Include all relevant details such as procedure and equipment numbers, product names and lot numbers
Apply the 5W2H method (What, When, Where, Who, Why if known, How much is involved, and How it was discovered)
Avoid speculation about causes in the initial description
Remember that the description should incorporate relevant records and photographs of discovered defects.
5W2H
Typical questions
Contains
Who?
Who are the people directly concerned with the problem? Who does this? Who should be involved but wasn’t? Was someone involved who shouldn’t be?
User IDs, Roles and Departments
What?
What happened?
Action, steps, description
When?
When did the problem occur?
Times, dates, place In process
Where?
Where did the problem occur?
Location
Why is it important?
Why did we do this? What are the requirements? What is the expected condition?
Justification, reason
How?
How did we discover. Where in the process was it?
Method, process, procedure
How Many? How Much?
How many things are involved? How often did the situation happen? How much did it impact?
Number, frequency
The quality of your deviation documentation begins with this initial identification. As I’ve emphasized in previous posts, the investigation/deviation report should tell a story that can be easily understood by all parties well after the event and the investigation. This narrative begins with clear identification on day one.
Elements
Problem Statement
Is used to…
Understand and target a problem. Providing a scope. Evaluate any risks. Make objective decisions
Answers the following… (5W2H)
What? (problem that occurred);When? (timing of what occurred); Where? (location of what occurred); Who? (persons involved/observers); Why? (why it matters, not why it occurred); How Much/Many? (volume or count); How Often? (First/only occurrence or multiple)
Contains…
Object (What was affected?); Defect (What went wrong?)
GEMBA-the actual place where work happens-is a cornerstone concept in quality management. When a deviation occurs, there is no substitute for being physically present at the location.
Observe the actual conditions and environment firsthand
Notice details that might not be captured in written reports
Understand the workflow and context surrounding the deviation
Gather physical evidence before it’s lost or conditions change
Create the opportunity for meaningful conversations with operators
Human error occurs because we are human beings. The extent of our knowledge, training, and skill has little to do with the mistakes we make. We tire, our minds wander and lose concentration, and we must navigate complex processes while satisfying competing goals and priorities – compliance, schedule adherence, efficiency, etc.
Foremost to understanding human performance is knowing that people do what makes sense to them given the available cues, tools, and focus of their attention at the time. Simply put, people come to work to do a good job – if it made sense for them to do what they did, it will make sense to others given similar conditions. The following factors significantly shape human performance and should be the focus of any human error investigation:
Physical Environment Environment, tools, procedures, process design
Organizational Culture Just- or blame-culture, attitude towards error
Management and Supervision Management of personnel, training, procedures
We do not want to see or experience human error – but when we do, it’s imperative to view it as a valuable opportunity to improve the system or process. This mindset is the heart of effective human error prevention.
Conducting an Effective GEMBA Walk for Deviations
When conducting your GEMBA walk specifically for deviation investigation:
Arrive with a clear purpose and structured approach
Observe before asking questions
Document observations with photos when appropriate
Look for environmental factors that might not appear in reports
Pay attention to equipment configuration and conditions
Note how operators interact with the process or equipment
A deviation gemba is a cross-functional team meeting that is assembled where a potential deviation event occurred. Going to the gemba and “freezing the scene” as close as possible to the time the event occurred will yield valuable clues about the environment that existed at the time – and fresher memories will provide higher quality interviews. This gemba has specific objectives:
Obtain a common understanding of the event: what happened, when and where it happened, who observed it, who was involved – all the facts surrounding the event. Is it a deviation?
Clearly describe actions taken, or that need to be taken, to contain impact from the event: product quarantine, physical or mechanical interventions, management or regulatory notifications, etc.
Interview involved operators: ask open-ended questions, like how the event unfolded or was discovered, from their perspective, or how the event could have been prevented, in their opinion – insights from personnel experienced with the process can prove invaluable during an investigation.
Deviation GEMBA Tips
Typically there is time between when notification of a deviation gemba goes out and when the team is scheduled to assemble. It is important to come prepared to help facilitate an efficient gemba:
Assemble procedures and other relevant documents and records. This will make references easier during the gemba.
Keep your team on-track – the gemba should end with the team having a common understanding of the event, actions taken to contain impact, and the agreed-upon next steps of the investigation.
You will gain plenty of investigational leads from your observations and interviews at the gemba – which documents to review, which personnel to interview, which equipment history to inspect, and more. The gemba is such an invaluable experience that, for many minor events, root cause and CAPA can be determined fairly easily from information gathered solely at the gemba.
Informal Rubric for Conducting a Good Deviation GEMBA
Describe the timeliness of the team gathering at the gemba.
Were all required roles and experts present?
Was someone leading or facilitating the gemba?
Describe any interviews the team performed during the gemba.
Did the team get sidetracked or off-topic during the gemba
Was the team prepared with relevant documentation or information?
Did the team determine batch impact and any reportability requirements?
Did the team satisfy the objectives of the gemba?
What did the team do well?
What could the team improve upon?
Speaking with Operators: The Power of Cognitive Interviewing
Interviewing personnel who were present when the deviation occurred requires special techniques to elicit accurate, complete information. Traditional questioning often fails to capture critical details.
Cognitive interviewing, as I outlined in my previous post on “Interviewing,” was originally created for law enforcement and later adopted during accident investigations by the National Transportation Safety Board (NTSB). This approach is based on two key principles:
Witnesses need time and encouragement to recall information
Retrieval cues enhance memory recall
How to Apply Cognitive Interviewing in Deviation Investigations
Mental Reinstatement: Encourage the interviewee to mentally recreate the environment and people involved
In-Depth Reporting: Encourage the reporting of all the details, even if it is minor or not directly related
Multiple Perspectives: Ask the interviewee to recall the event from others’ points of view
Several Orders: Ask the interviewee to recount the timeline in different ways. Beginning to end, end to beginning
Most importantly, conduct these interviews at the actual location where the deviation occurred. A key part of this is that retrieval cues access memory. This is why doing the interview on the scene (or Gemba) is so effective.
Component
What It Consists of
Mental Reinstatement
Encourage the interviewee to mentally recreate the environment and people involved.
In-Depth Reporting
Encourage the reporting of all the details.
Multiple Perspectives
Ask the interviewee to recall the event from others’ points of view.
Several Orders
Ask the interviewee to recount the timeline in different ways.
Approach the Interviewee Positively:
Ask for the interview.
State the purpose of the interview.
Tell interviewee why he/she was selected.
Avoid statements that imply blame.
Focus on the need to capture knowledge
Answer questions about the interview.
Acknowledge and respond to concerns.
Manage negative emotions.
Apply these Four Components:
Use mental reinstatement.
Report everything.
Change the perspective.
Change the order.
Apply these Two Principles:
Witnesses need time and encouragement to recall information.
Retrieval cues enhance memory recall.
Demonstrate these Skills:
Recreate the original context and had them walk you through process.
Tell the witness to actively generate information.
Adopt the witness’s perspective.
Listen actively, do not interrupt, and pause before asking follow-up questions.
Ask open-ended questions.
Encourage the witness to use imagery.
Perform interview at the Gemba.
Follow sequence of the four major components.
Bring support materials.
Establish a connection with the witness.
Do Not tell them how they made the mistake.
Initial Impact Assessment: Understanding the Scope
Within the first 24 hours, a preliminary impact assessment is essential for determining the scope of the deviation and the appropriate response.
Apply a risk-based approach to categorize the deviation as critical, major, or minor
Evaluate all potentially affected products, materials, or batches
Consider potential effects on critical quality attributes
Assess possible regulatory implications
Determine if released products may be affected
This impact assessment is also the initial risk assessment, which will help guide the level of effort put into the deviation.
Factors to Consider in Initial Risk Assessment
Patient safety implications
Product quality impact
Compliance with registered specifications
Potential for impact on other batches or products
Regulatory reporting requirements
Level of investigation required
This initial assessment will guide subsequent decisions about quarantine, notification requirements, and the depth of investigation needed. Remember, this is a preliminary assessment that will be refined as the investigation progresses.
Immediate Actions: Containing the Issue
Once you’ve identified the deviation and assessed its potential impact, immediate actions must be taken to contain the issue and prevent further risk.
Quarantine potentially affected products or materials to prevent their release or further use
Notify key stakeholders, including quality assurance, production supervision, and relevant department heads
Implement temporary corrective or containment measures
Document the deviation in your quality management system
Secure relevant evidence and documentation
Consider whether to stop related processes
Industry best practices emphasize that you should Report the deviation in real-time. Notify QA within 24 hours and hold the GEMBA. Remember that “if you don’t document it, it didn’t happen” – thorough documentation of both the deviation and your immediate response is essential.
Affected vs Related Batches
Not every Impact is the same, so it can be helpful to have two concepts: Affected and Related.
Affected Batch: Product directly impacted by the event at the time of discovery, for instance, the batch being manufactured or tested when the deviation occurred.
Related Batch: Product manufactured or tested under the same conditions or parameters using the process in which the deviation occurred and determined as part of the deviation investigation process to have no impact on product quality.
Setting Up for a Successful Full Investigation
The final step in the golden day is establishing the foundation for the comprehensive investigation that will follow.
Assemble a cross-functional investigation team with relevant expertise
Define clear roles and responsibilities for team members
Establish a timeline for the investigation (remembering the 30-day guideline)
Identify additional data or evidence that needs to be collected
Plan for any necessary testing or analysis
Schedule follow-up interviews or observations
In my post on handling deviations, I emphasized that you must perform a time-sensitive and thorough investigation within 30 days. The groundwork laid during the golden day will make this timeline achievable while maintaining investigation quality.
Planning for Root Cause Analysis
During this setup phase, you should also begin planning which root cause analysis tools might be most appropriate for your investigation. Select tools based on the event complexity and the number of potential root causes and when “human error” appears to be involved, prepare to dig deeper as this is rarely the true root cause
Identifying Phase of your Investigation
If
Then you are at
The problem is not understood. Boundaries have not been set. There could be more than one problem
Problem Understanding
Data needs to be collected. There are questions about frequency or occurrence. You have not had interviews
Data Collection
Data has been collected but not analyszed
Data Analysis
The root cause needs to be determined from the analyzed data
A picture of the separate steps of a process in sequential order, including:
materials or services entering or leaving the process (inputs and outputs)
decisions that must be made
people who become involved
time involved at each step, and/or
process measurements.
Critical Incident Technique (CIT)
A process used for collecting direct observations of human behavior that
have critical significance, and
meet methodically defined criteria.
Comparative Analysis
A technique that focuses a problem-solving team on a problem. It compares one or more elements of a problem or process to evaluate elements that are similar or different (e.g. comparing a standard process to a failing process).
Performance Matrix
A tool that describes the participation by various roles in completing tasks or deliverables for a project or business process. Note: It is especially useful in clarifying roles and responsibilities in cross-functional/departmental positions.
5W2H Analysis
An approach that defines a problem and its underlying contributing factors by systematically asking questions related to who, what, when, where, why, how, and how much/often.
Data Collection
Surveys
A technique for gathering data from a targeted audience based on a standard set of criteria.
Check Sheets
A technique to compile data or observations to detect and show trends/patterns.
Cognitive Interview
An interview technique used by investigators to help the interviewee recall specific memories from a specific event.
KNOT Chart
A data collection and classification tool to organize data based on what is
Known
Need to know
Opinion, and
Think we know.
Data Analysis
Pareto Chart
A technique that focuses efforts on problems offering the greatest potential for improvement.
Histogram
A tool that
summarizes data collected over a period of time, and
graphically presents frequency distribution.
Scatter Chart
A tool to study possible relationships between changes in two different sets of variables.
Run Chart
A tool that captures study data for trends/patterns over time.
Affinity Diagram
A technique for brainstorming and summarizing ideas into natural groupings to understand a problem.
Root Cause Analysis
Interrelationship Digraphs
A tool to identify, analyze, and classify cause and effect relationships among issues so that drivers become part of an effective solution.
Why-Why
A technique that allows one to explore the cause-and-effect relationships of a particular problem by asking why; drilling down through the underlying contributing causes to identify root cause.
Is/Is Not
A technique that guides the search for causes of a problem by isolating the who, what, when, where, and how of an event. It narrows the investigation to factors that have an impact and eliminates factors that do not have an impact. By comparing what the problem is with what the problem is not, we can see what is distinctive about a problem which leads to possible causes.
Structured Brainstorming
A technique to identify, explore, and display the
factors within each root cause category that may be affecting the problem/issue, and/or
effect being studied through this structured idea-generating tool.
Cause and Effect Diagram (Ishikawa/Fishbone)
A tool to display potential causes of an event based on root cause categories defined by structured brainstorming using this tool as a visual aid.
Causal Factor Charting
A tool to
analyze human factors and behaviors that contribute to errors, and
identify behavior-influencing factors and gaps.
Other Tools
Prioritization Matrix
A tool to systematically compare choices through applying and weighting criteria.
Control Chart
A tool to monitor process performance over time by studying its variation and source.
Process Capability
A tool to determine whether a process is capable of meeting requirements or specifications.
Making the Most of Your Golden Day
The first 24 hours after discovering a deviation represent a unique opportunity that should not be wasted. By following the structured approach outlined in this post-identifying the problem clearly, going to the GEMBA, interviewing operators using cognitive techniques, conducting an initial impact assessment, taking immediate containment actions, and setting up for the full investigation-you maximize the value of this golden day.
Remember that excellent deviation management is directly linked to product quality, patient safety, and regulatory compliance. Each well-managed deviation is an opportunity to strengthen your quality system.
I encourage you to assess your current approach to the first 24 hours of deviation management. Are you capturing the full value of this golden day, or are you letting critical information slip away? Implement these strategies, train your team on proper deviation triage, and transform your deviation response from reactive to proactive.
Your deviation management effectiveness doesn’t begin when the investigation report is initiated-it begins the moment a deviation is discovered. Make that golden day count.
Psychological safety refers to a shared belief among team members that they are safe to take risks, share their thoughts, and learn from their mistakes without fear of negative consequences. This concept is foundational to building a culture where individuals feel valued, included, and motivated to contribute their unique perspectives. It is the bedrock upon which effective collaboration, creativity, and problem-solving are built. In environments where psychological safety is prioritized, employees are more likely to engage in open dialogue, admit mistakes, and explore new ideas, leading to enhanced innovation and productivity.
The Role of Leadership in Fostering Psychological Safety
Effective leadership plays a pivotal role in establishing and maintaining a culture of psychological safety. Leaders must set the tone by modeling vulnerability, encouraging open communication, and demonstrating empathy towards their team members. They should establish clear expectations of respect and inclusivity, ensuring that diverse perspectives are welcomed and valued. By doing so, leaders create an environment where employees feel comfortable sharing their thoughts and ideas, which is essential for driving innovation and solving complex problems.
In the past post on Psychological Safety, Reflexivity, and Problem Solving, I explored how psychological safety enables individuals to behave authentically and express themselves candidly, which is crucial for effective problem-solving and reflexivity in organizations. This authenticity allows teams to tackle challenges more effectively by leveraging diverse viewpoints and experiences.
Building a Quality Culture
A quality culture is deeply intertwined with psychological safety. It emphasizes continuous improvement, learning from mistakes, and a commitment to excellence. In such a culture, employees are encouraged to reflect on their processes, identify areas for improvement, and implement changes that enhance overall performance. This reflective practice is facilitated by psychological safety, as it allows individuals to share insights and ideas without fear of criticism, thereby fostering a collaborative and adaptive environment.
Strategies for Creating a Safe Space for Reflection
Creating a safe space for reflection involves several strategic steps:
Establishing Open Communication Channels
Organizations should implement transparent and constructive communication channels that allow employees to express their thoughts, concerns, and ideas without fear of negative consequences. This can be achieved through regular team meetings, anonymous feedback systems, or open forums where employees feel comfortable sharing their perspectives. Active listening and empathy are crucial in these interactions, as they reinforce the sense of safety and encourage further participation.
Implementing Psychological Safety Training
Providing comprehensive training on psychological safety is essential for building awareness and equipping employees with the skills needed to navigate complex interactions and support their colleagues. These programs should emphasize the importance of trust, vulnerability, and inclusivity, and offer practical strategies for fostering a psychologically safe environment. By educating employees on these principles, organizations can ensure that psychological safety becomes an integral part of their culture.
Encouraging Active Participation and Feedback
Encouraging active participation involves creating opportunities for employees to engage in collaborative discussions and provide feedback. This can be facilitated through workshops, brainstorming sessions, or project meetings where diverse perspectives are sought and valued. Feedback loops should be open and constructive, allowing employees to learn from their experiences and grow professionally.
Measuring Psychological Safety
Measuring psychological safety is critical for understanding its impact on organizational culture and identifying areas for improvement. This can be achieved through surveys, behavioral indicators, and engagement scores. Surveys should include questions that assess employees’ perceptions of safety, trust, and openness within their teams. Behavioral indicators, such as the frequency of idea sharing and openness in feedback loops, can also provide valuable insights into the level of psychological safety within an organization.
In our previous discussions on on this blog, I have emphasized the importance of a culture that supports open dialogue and continuous improvement. A few examples include:
“Change Strategies for Accelerating Change“: This post discusses strategies such as promoting cross-functional training, fostering informal interactions, and implementing feedback loops. These strategies are crucial for creating a culture that supports open dialogue and continuous improvement.
“Reducing Subjectivity in Quality Risk Management: Aligning with ICH Q9(R1)“: This post focuses on reducing subjectivity through structured approaches and data-driven decision-making. It underscores the importance of a culture that encourages open communication to ensure that decisions are based on comprehensive data rather than personal biases.
These examples illustrate the importance of fostering a culture that supports open dialogue and continuous improvement in complex industries.
Overcoming Challenges
Despite the benefits of psychological safety, several challenges may arise when attempting to implement it within an organization. Fear and resistance to change are common obstacles, particularly in hierarchical structures where speaking up can be perceived as risky. To overcome these challenges, organizations should identify influential champions who can model psychological safety behaviors and inspire others to do the same. Regular assessments and feedback sessions can also help identify areas where psychological safety is lacking, allowing for targeted interventions.
Sustaining Psychological Safety
Sustaining a culture of psychological safety requires ongoing effort and commitment. Organizations must regularly assess the effectiveness of their psychological safety initiatives and refine their strategies based on feedback and performance data. This involves ensuring that leadership behaviors consistently reinforce psychological safety principles and that training programs are scaled to reach all levels of the organization.
Conclusion
Building a safe space for reflection within an organization is a multifaceted process that relies heavily on psychological safety and a quality culture. By fostering an environment where employees feel valued, included, and empowered to share their ideas, organizations can unlock their full potential and drive innovation. Psychological safety is not a static state but a continuous journey that requires leadership commitment, effective communication, and ongoing evaluation. As we continue to navigate the complexities of modern organizational challenges, prioritizing psychological safety will remain essential for creating a workplace where employees thrive and contribute meaningfully.
By embracing psychological safety and fostering a quality culture, organizations can create a safe space for reflection that drives innovation, enhances collaboration, and promotes continuous improvement. This approach not only benefits the organization but also contributes to the well-being and growth of its employees, ultimately leading to a more resilient and adaptive workforce.